Downloaded 2,895 times


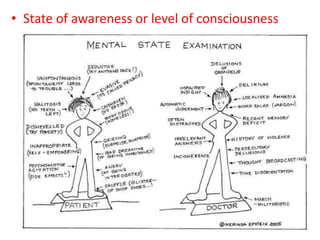



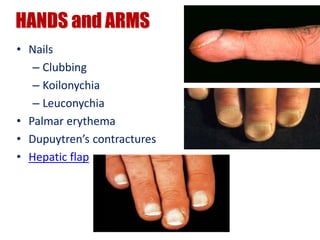
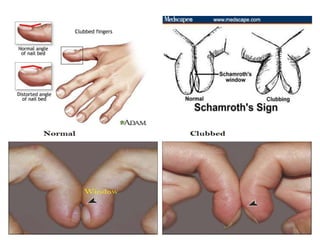





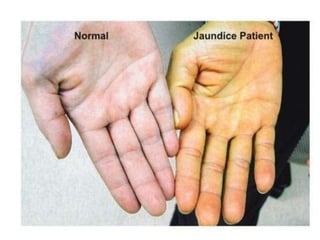


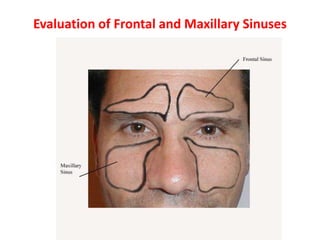
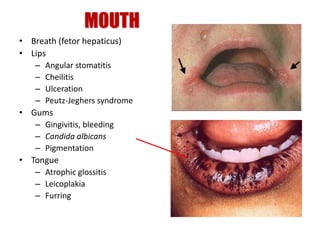
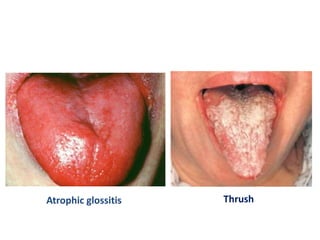



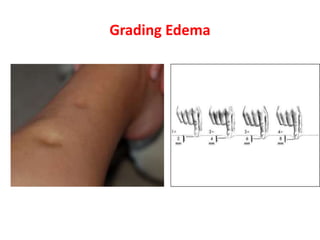
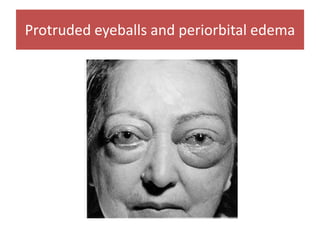
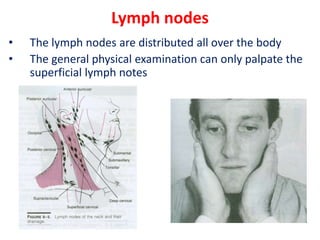
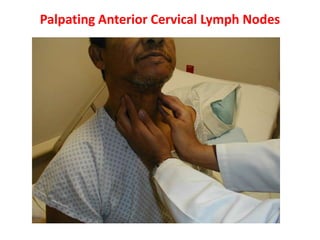


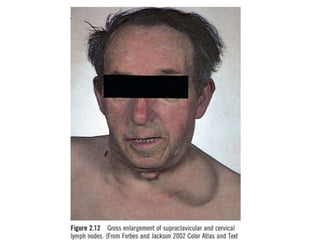
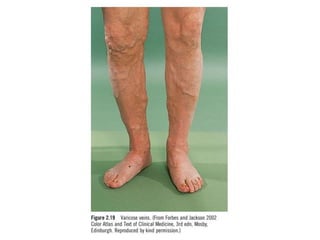
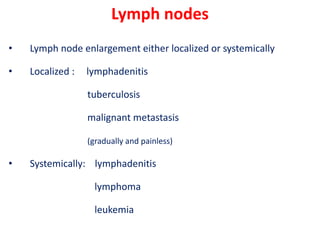
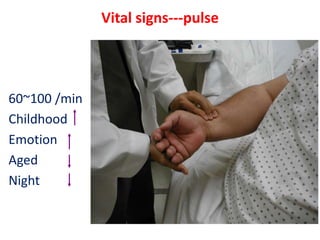


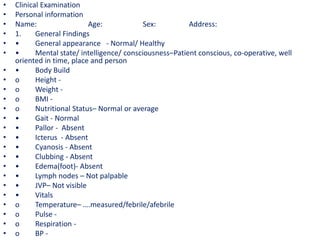

The document provides guidelines for conducting a clinical examination, including sections on vital data collection, general examination, and systemic examination. The general examination involves inspection of the general appearance, hands/arms, skin, face, eyes, mouth, neck, edema, lymph nodes, and vital signs. Specific signs and abnormalities are described for different body systems and diseases. The guidelines emphasize the importance of thorough history taking and physical examination for making accurate diagnoses.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















