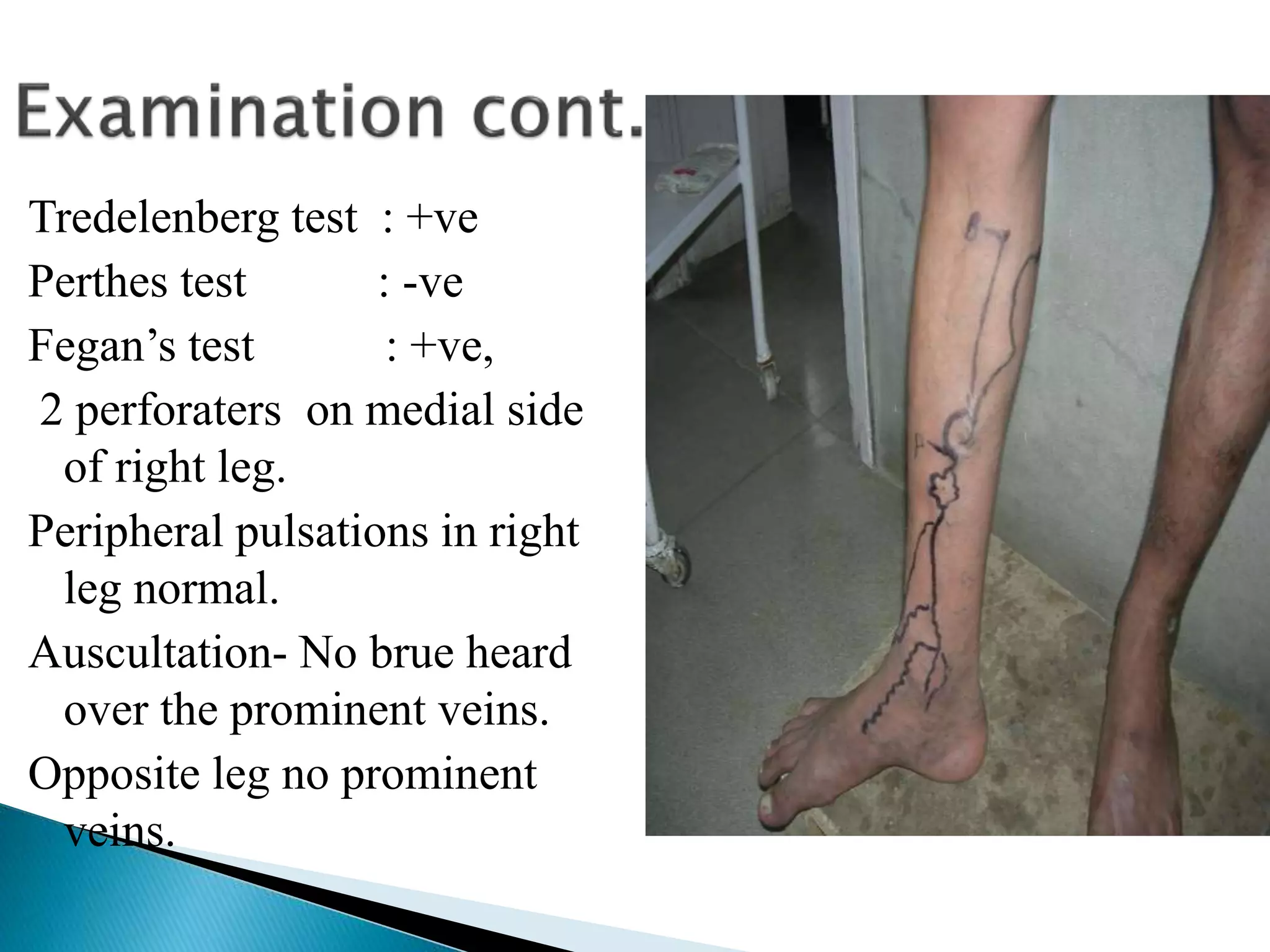
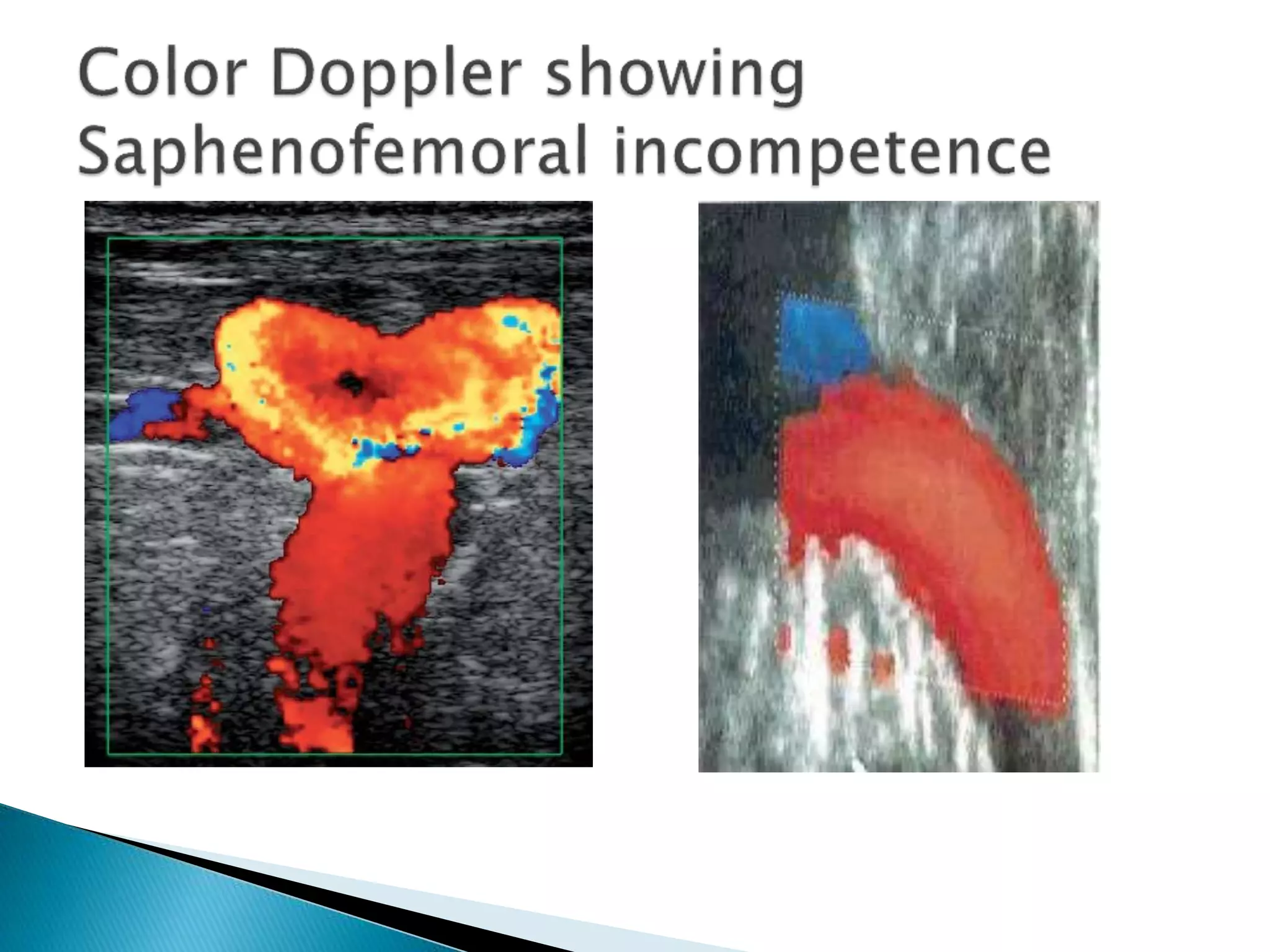
This document describes a 32-year-old male farmer who presented with prominent veins in his right leg for 2 years along with swelling and pain in the right leg for 1 year. On examination, dilated veins were visible on the medial side of the right leg, ankle, and foot extending to the thigh. Tests showed saphenofemoral and perforator incompetence on the right side. The diagnosis was clinical grade 4 varicose veins. Color doppler ultrasound was recommended to further evaluate the perforators and veins, and pre-anaesthetic tests were ordered prior to a planned surgery involving high saphenofemoral junction ligation and stripping of the long saphenous vein along with ligation of perforators and