Downloaded 1,333 times






























































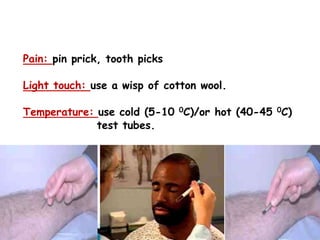





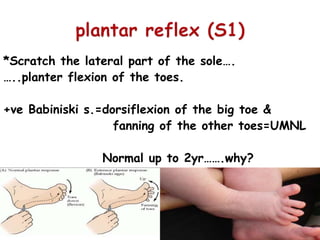














This document provides an overview of the pediatric examination process. It discusses examining various body systems including: 1. Mental status and neurological assessment including cranial nerves, motor and sensory systems, and reflexes. 2. Assessment of consciousness, behavior, intelligence, memory, and speech. 3. Evaluation of muscle tone, power, involuntary movements, and coordination. 4. Sensory testing including superficial sensations, deep sensations, and cortical sensations. 5. Assessment of various reflexes including superficial, deep, and visceral reflexes. The summary outlines the key areas addressed in a comprehensive pediatric examination.






























































































