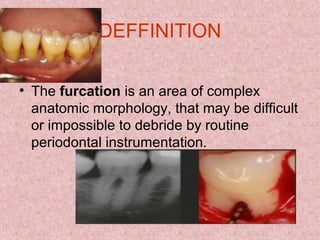
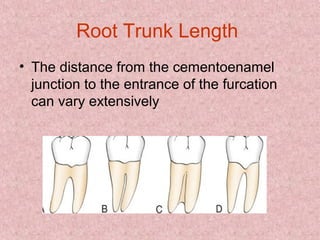
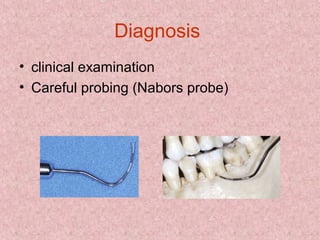
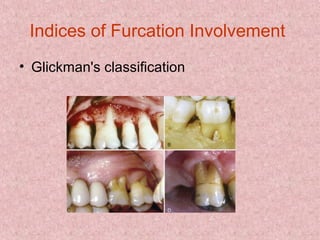




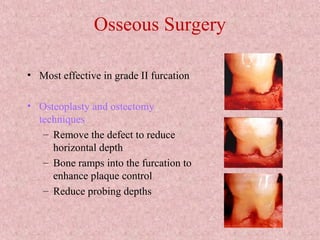
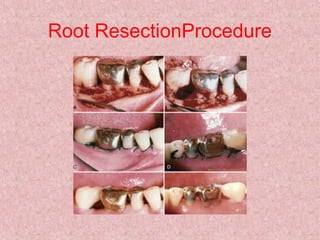
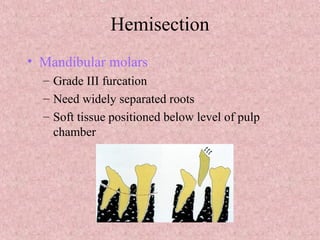


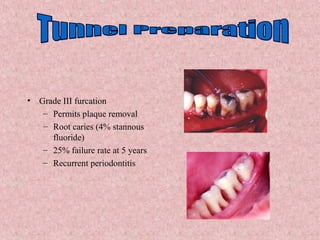


The document discusses furcation, which refers to the anatomical area where tooth roots divide. It defines furcation as a complex area that is difficult to clean. Factors like root anatomy, length, and enamel projections can influence furcation involvement. Furcation involvement is graded on a scale from I-IV based on probing depth and bone loss. Nonsurgical treatments include scaling and root planing while surgical options range from osseous resection to hemisection depending on the grade. Prognosis is best when thorough diagnosis and treatment are combined with good oral hygiene.
















































































