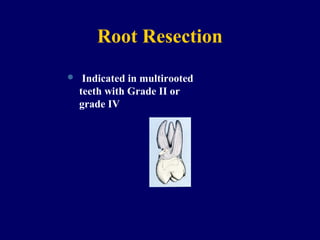
This document discusses furcation involvement and its classification and treatment. It defines furcation as an area of complex anatomy that is difficult to clean. Furcation involvement usually results from periodontal disease affecting the root trunk where two or more roots meet. It describes Glickman's classification of furcation from Class I to IV, based on the degree of bone and soft tissue loss. Treatment options discussed include non-surgical root preparation, antimicrobials, open debridement, surgical treatments like osseous resection, root resection, hemisection, regeneration, grafts, and extraction. Maintaining furcated teeth requires eliminating plaque and establishing anatomy to facilitate cleaning.