Downloaded 2,123 times
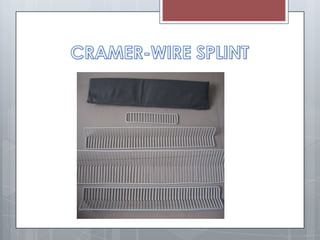
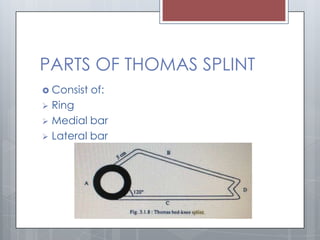
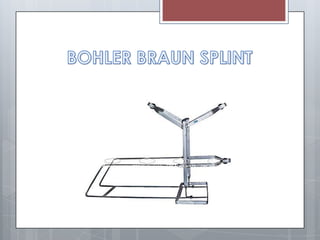
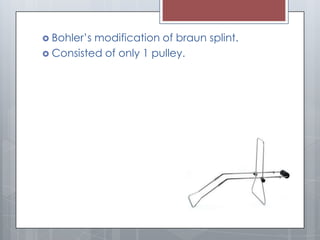





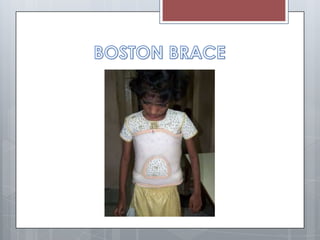

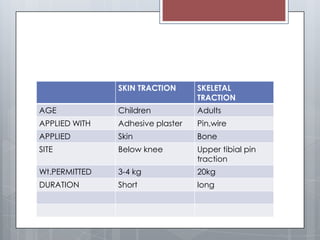


This document discusses different types of splints and traction used for immobilizing fractures. It describes ladder splints, Thomas splints, and Bohler's modification of the Braun splint. Thomas splints consist of a ring, medial bar, and lateral bar and are used to immobilize the lower limb. Bohler's modification uses pulleys to allow changing the angle of traction without adjusting the traction arrangement. The document also covers skin traction versus skeletal traction, application sites for each, and risks associated with traction use.