● MAIN PURPOSE:prevent further
trauma and reduce pain
● Almost any rigid material can be used as
a splint in emergency
“SPLINT IS ANY RIGID DEVICE USED TO IMMOBILIZE THE INJURED
PART OF THE BODY”
4.
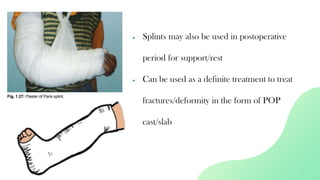
● Splints mayalso be used in postoperative
period for support/rest
● Can be used as a definite treatment to treat
fractures/deformity in the form of POP
cast/slab
5.
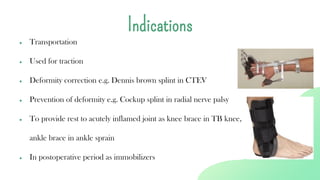
● Transportation
● Usedfor traction
● Deformity correction e.g. Dennis brown splint in CTEV
● Prevention of deformity e.g. Cockup splint in radial nerve palsy
● To provide rest to acutely inflamed joint as knee brace in TB knee,
ankle brace in ankle sprain
● In postoperative period as immobilizers
Indications
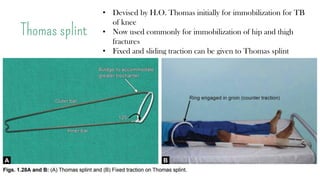
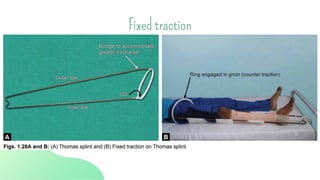
Thomas splint
• Devisedby H.O. Thomas initially for immobilization for TB
of knee
• Now used commonly for immobilization of hip and thigh
fractures
• Fixed and sliding traction can be given to Thomas splint
8.
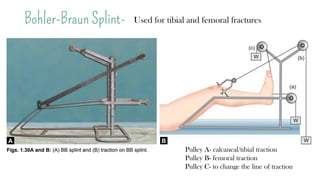
Bohler-Braun Splint-
Pulley A-calcaneal/tibial traction
Pulley B- femoral traction
Pulley C- to change the line of traction
Used for tibial and femoral fractures
● Splint mustbe applied properly and adequately padded at bony prominences and
fracture site
● Bandage of the splint mustn’t be too tight nor too loose
● Patient must be encouraged to exercise the muscles actively and the joints inside the
splint as much as permitted
● Any compression of nerve/vessel (tight bandage/inadequate padding) should be
detected early and managed
Care of a patient in a splint
11.
● Daily checkingand adjustments if required should be made and regular x-rays
should be taken to ensure good position of the fracture
● Assessment of compartment pressure- Always keep an eye on development of
compartment syndrome (Dx made on clinical suspicion of tense swelling and
pain on passive stretching of a limb)
● Encourage active toe/finger movement to reduce swelling
Care of a patient in a splint
TRACTIONS
❑ Traction countersforces that doesn’t allow
reduction/alignment to happen
❑ Traction is applied to the limb distal to the fracture—exert a
continuous pull in the long axis of the bone with a
counterforce in the opposite direction
14.
❑ It shouldalways be opposed by counter traction otherwise it
merely pulls the patient off the bed
❑ Traction requires constant care and vigilance and is
associated with hazards of prolonged bed rest
❑ In modern orthopedics, traction is generally used as a
temporary measure to bridge the time from fracture to
definite treatment
15.
● Immobilization ofa painful, inflamed joint/ fractures
● To achieve a normal anatomical orientation in cases of fractures and
dislocations when surgery is delayed or not possible due to medical
reasons
● To reduce muscle spasms, deformities and relieve pain
● Correction of soft tissue contractures by stretching them out
Indications of traction
16.
FIXED TRACTION
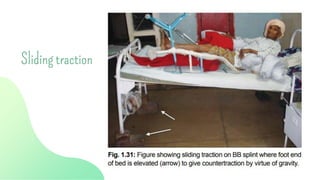
SLIDING/BALANCED TRACTION
TYPESOF TRACTION
• Counter-traction is provided by the traction system itself over a
body part
• Weight of the body acts as counter-traction, made effective by
elevating the foot end of the bed
COMBINED TRACTION
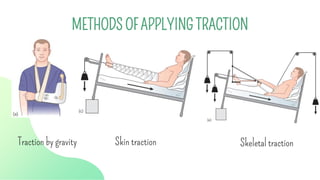
METHODS OF APPLYINGTRACTION
Traction by gravity Skin traction Skeletal traction
20.
❑ Only applicablefor upper limb injuries
❑ With a wrist sling the weight of the arm
provides continuous traction to the humerus
TRACTION BY GRAVITY
21.
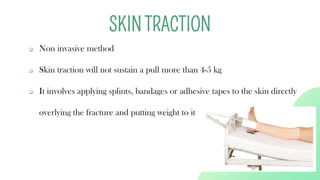
❑ Non invasivemethod
❑ Skin traction will not sustain a pull more than 4-5 kg
❑ It involves applying splints, bandages or adhesive tapes to the skin directly
overlying the fracture and putting weight to it
SKIN TRACTION
22.
❑ Skin allergiesfrom adhesive material
❑ Skin excoriation
❑ Abrasions to the skin
❑ Pressure sores
❑ Compression of superficial nerves (adequate padding is necessary)
Complications of skin traction
23.
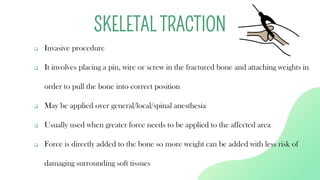
❑ Invasive procedure
❑It involves placing a pin, wire or screw in the fractured bone and attaching weights in
order to pull the bone into correct position
❑ May be applied over general/local/spinal anesthesia
❑ Usually used when greater force needs to be applied to the affected area
❑ Force is directly added to the bone so more weight can be added with less risk of
damaging surrounding soft tissues
SKELETAL TRACTION
● Adverse reactionto anesthesia
● Bleeding from pin tract site
● Infection of the pin tract
● Damage to the surrounding tissues
● Neurovascular injury by the pin insertion
● Hazards of prolonged bed rest
Complications of skeletal traction
27.
Which traction toapply?
❑ Skin traction should be used as whenever possible
❑ If traction is required for immobilization and
surgery is planned soon, skin traction is ideal
❑ If >5 kg weight is needed skin traction cant be used
❑ For reduction purpose, minimum weight required
is 10% of the body weight so skeletal traction is
ideal
28.
● Traction shouldbe as comfortable as possible
● Proper functioning of the traction unit must be ensured and traction weights
must not touch the ground
● Terminal part of the limb in traction must be warm, of normal color and
with intact sensations (tingling/numbness- traction palsy of the nerve)
● Any swelling must be checked (tight bandage/slipped skin traction)
Care of a patient in traction
29.
● Pain ongentle tapping at the site of pin insertion may signify pin tract
infection
● Proper position of fracture should be ensured by taking x-rays in
traction
● Physiotherapy must be continued to minimize muscle wasting
● Watch out complications of prolonged bed rest like bed sores,
thromboembolism, constipation etc,
Care of a patient in traction
30.
References
● Fundamentals ofOrthopedics, Mukul Mohindra, 1st Edition, 2016
● Apley and Solomon’s System of Orthopaedics and Trauma, 10th Edition
● Essential Orthopaedics, 6th Edition
● MBBS Viva Made Easy by Dr. Amit Joshi, 2nd Edition




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
