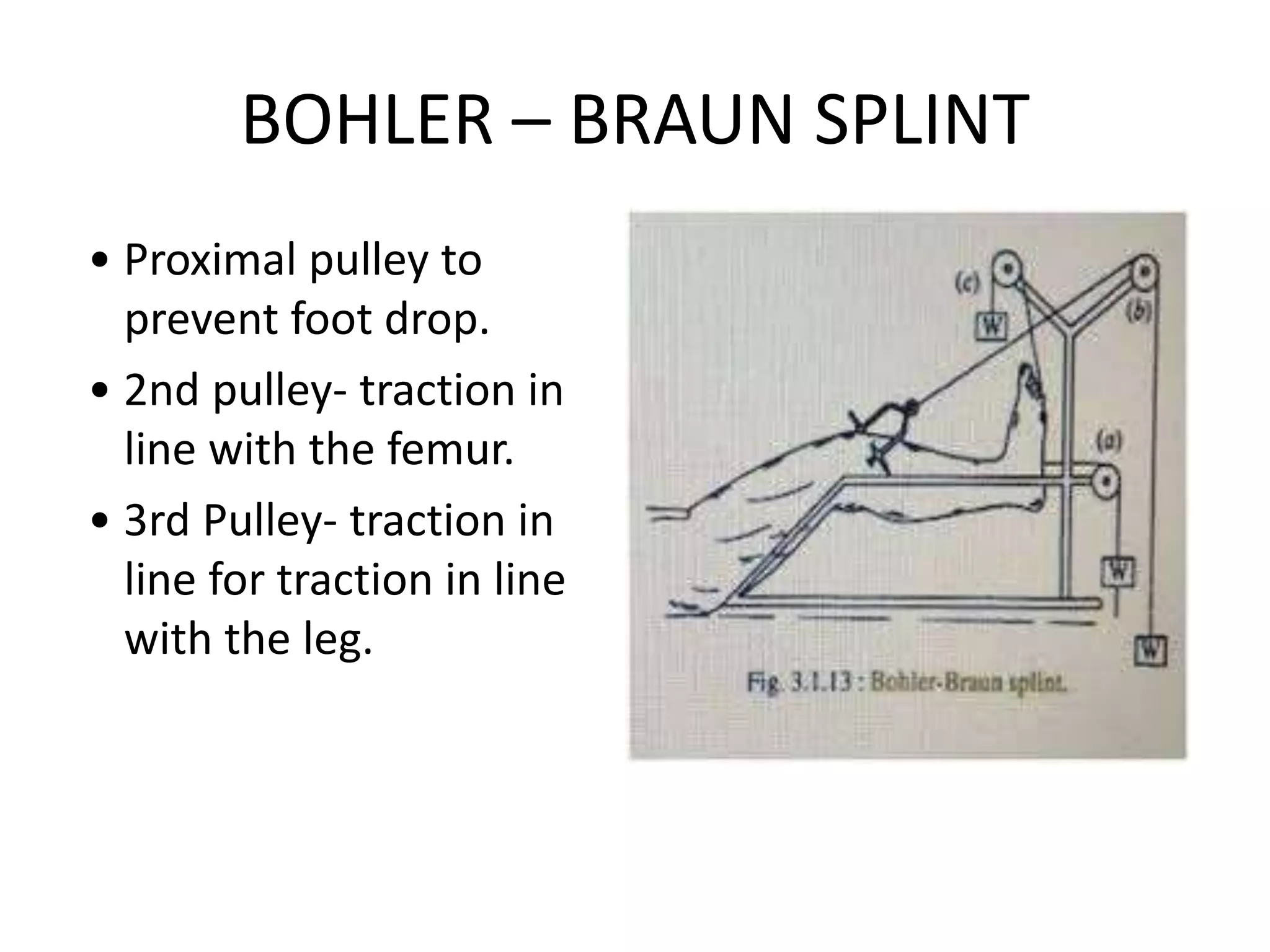
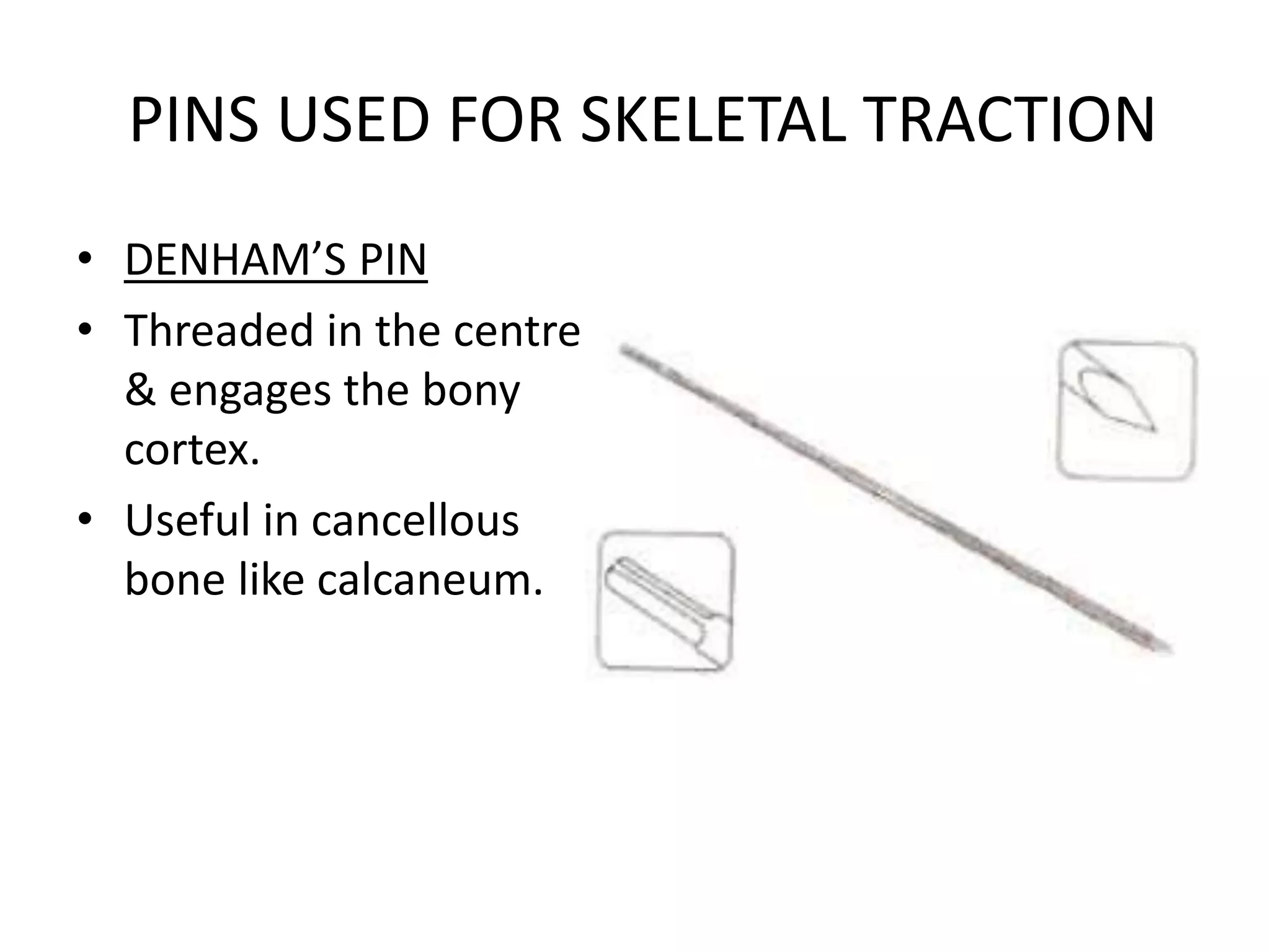
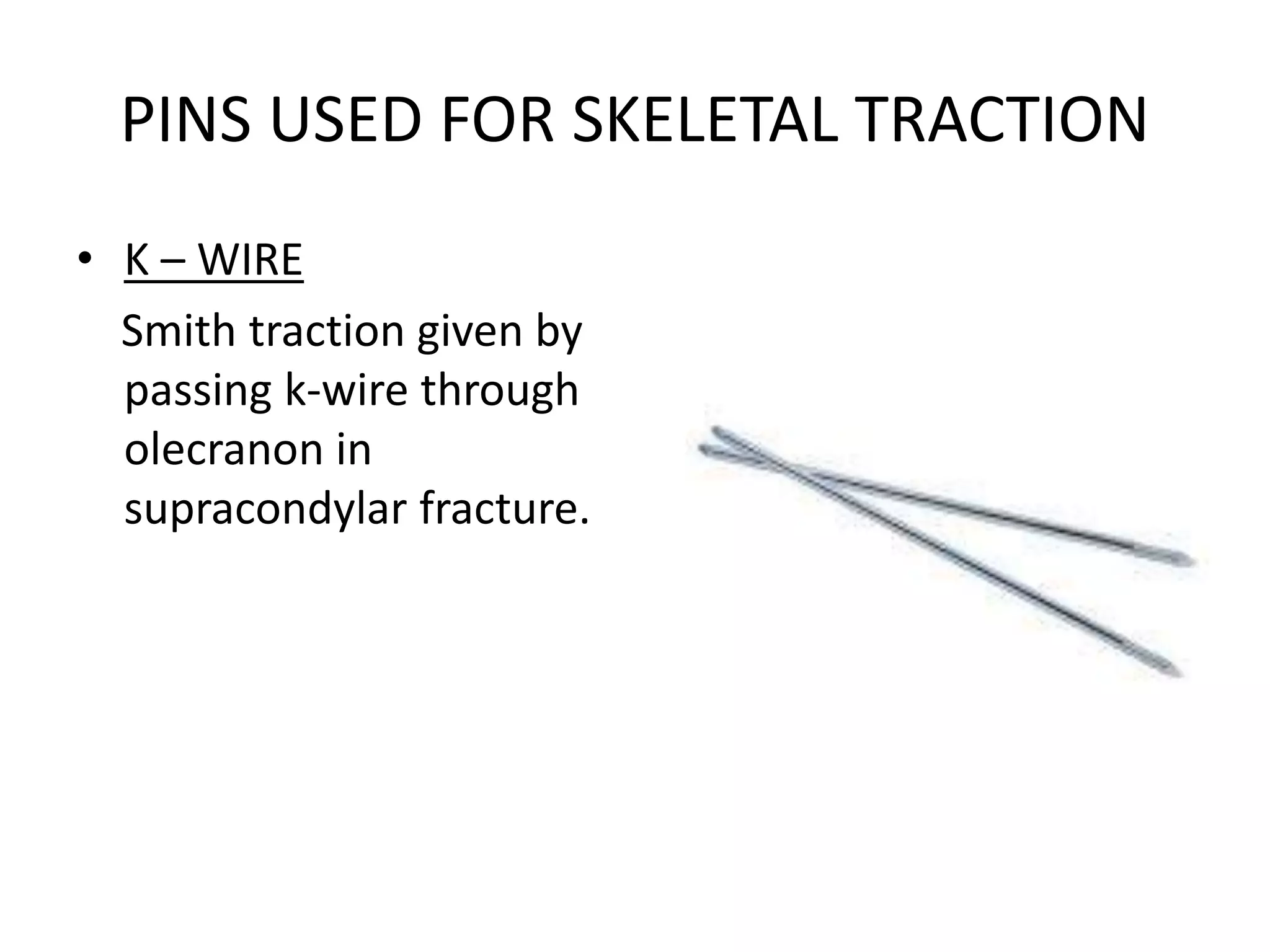
This document discusses splints and tractions used in orthopedics. It describes various types of splints like POP, Thomas splint, Bohler-Braun splint, and braces. POP splints are cheap, easily available and comfortable. Thomas splints are used to immobilize the knee. Traction is used to restore alignment to fractures and reduce pain. There are different types of traction like skin traction and skeletal traction applied using pins. Daily care of patients involves ensuring proper traction and preventing complications.