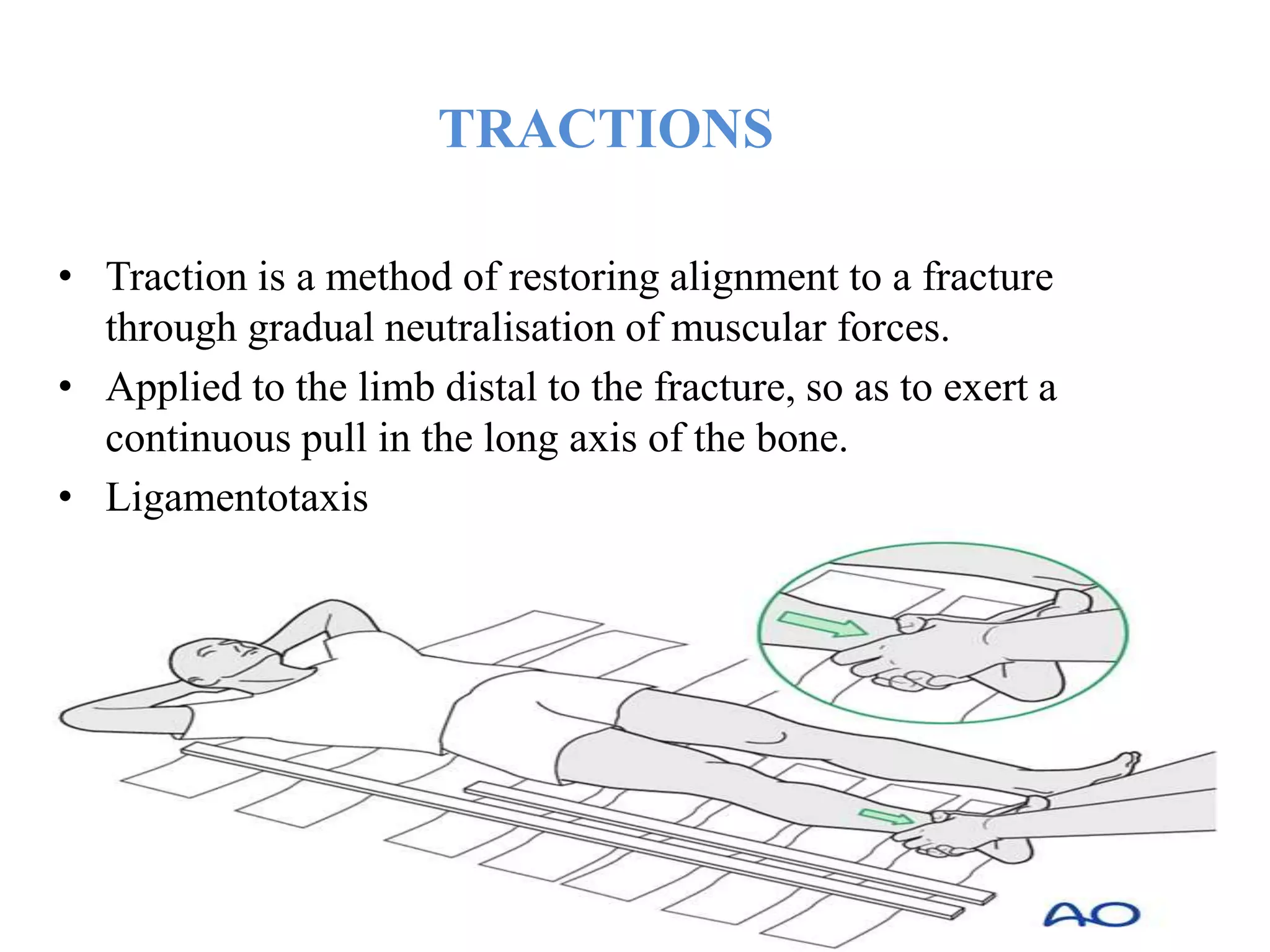
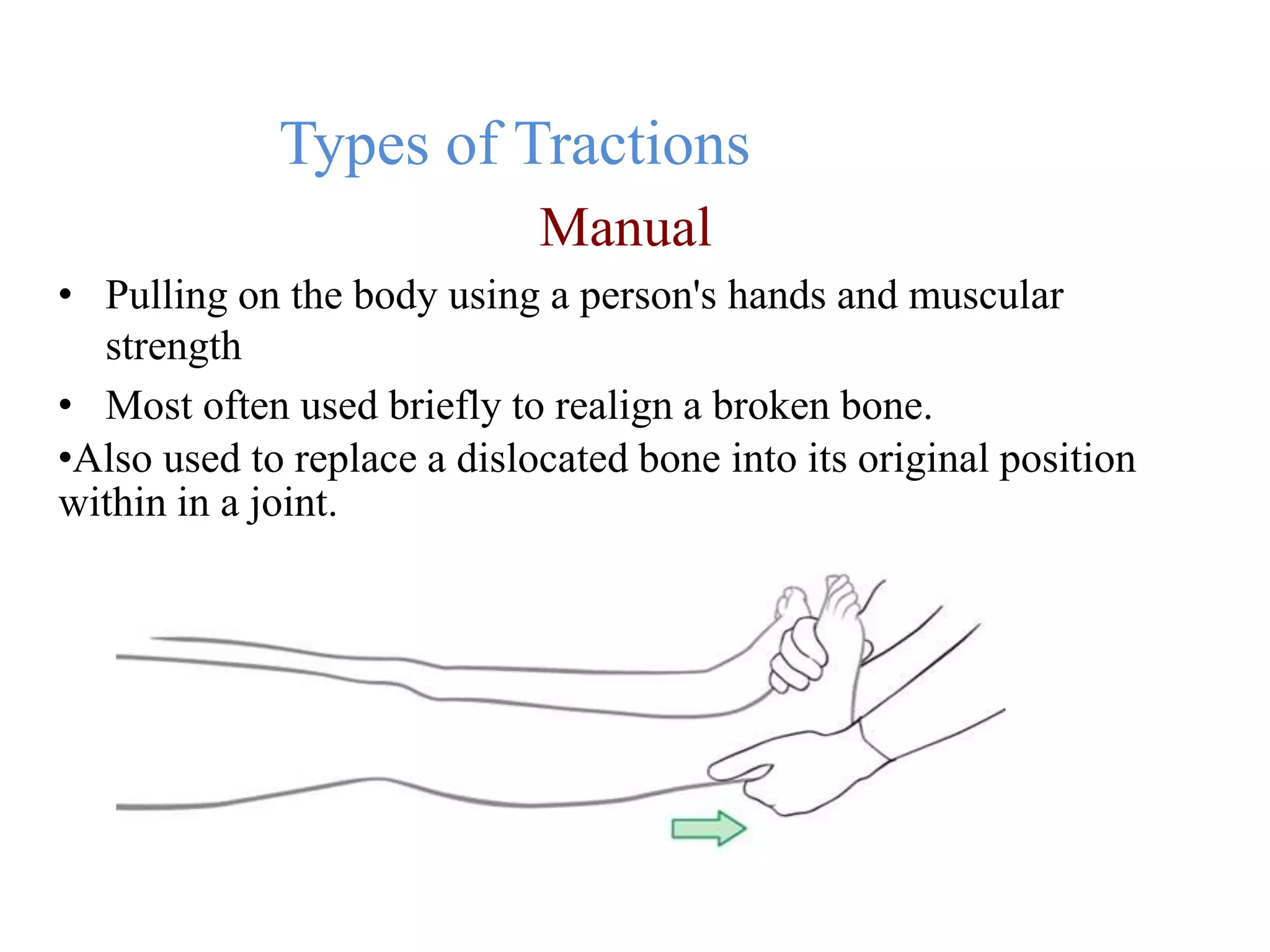
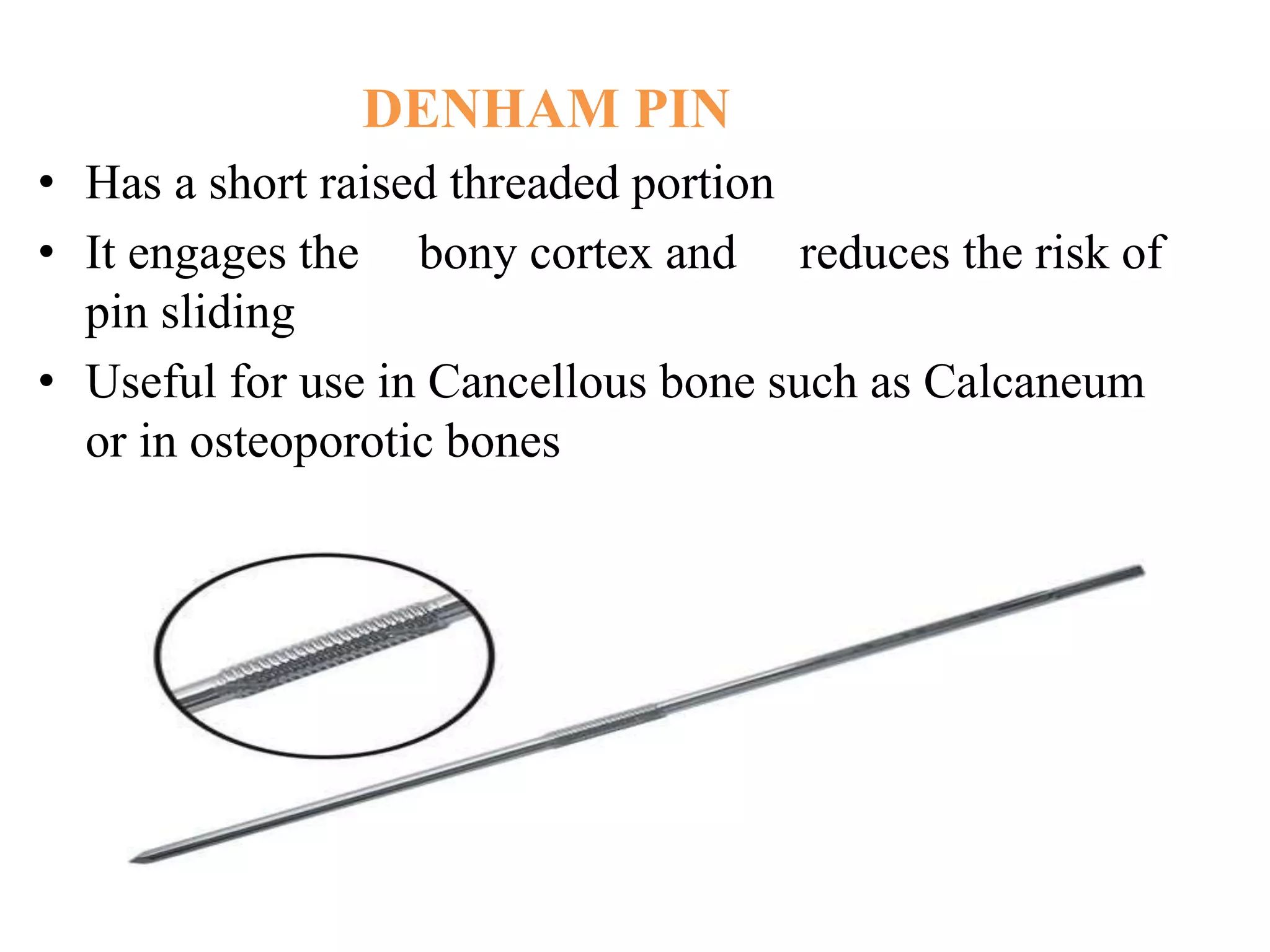
This document discusses various types of splints and tractions used in orthopedics. It begins by defining a splint and its functions, which include immobilization, pain control, and prevention of further injury. It describes different types of splints like the Thomas splint and Bohler-Braun splint. Traction is defined as a method of restoring bone alignment through gradual neutralization of muscles. Different traction types include skin, skeletal, and pelvic traction. Complications of splinting and traction are also outlined. The document provides detailed information on preparation, applications, and care for a variety of splints and traction techniques.




























































































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)































