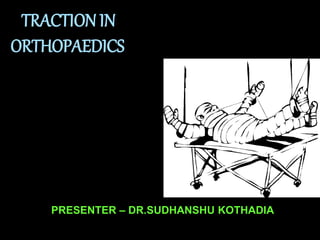
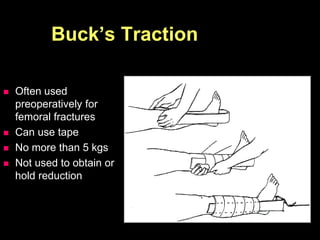
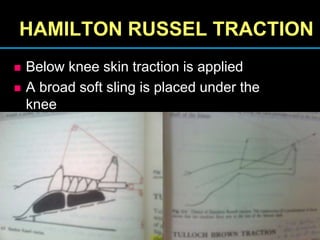
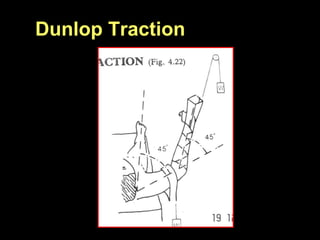
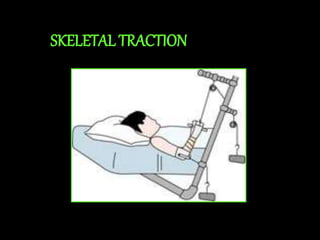
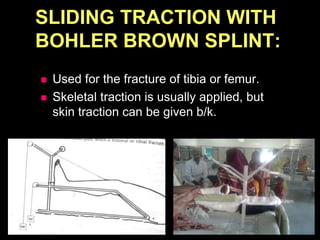
Traction is used to stretch or align bones and relieve pressure on joints and nerves. There are two main types - fixed traction which uses a fixed point of counterpressure, and sliding traction which uses gravity. Skin traction applies force over a large skin area while skeletal traction uses pins inserted into bones. Common sites for skeletal traction include the proximal tibia, distal tibia, and calcaneus. Traction is used to treat fractures, deformities, joint inflammation and pain. Precautions must be taken to prevent complications like infection, nerve injury, or distraction at the fracture site.