The document provides information about plaster of Paris casts, including their history, composition, application process, types, and care. Some key points:
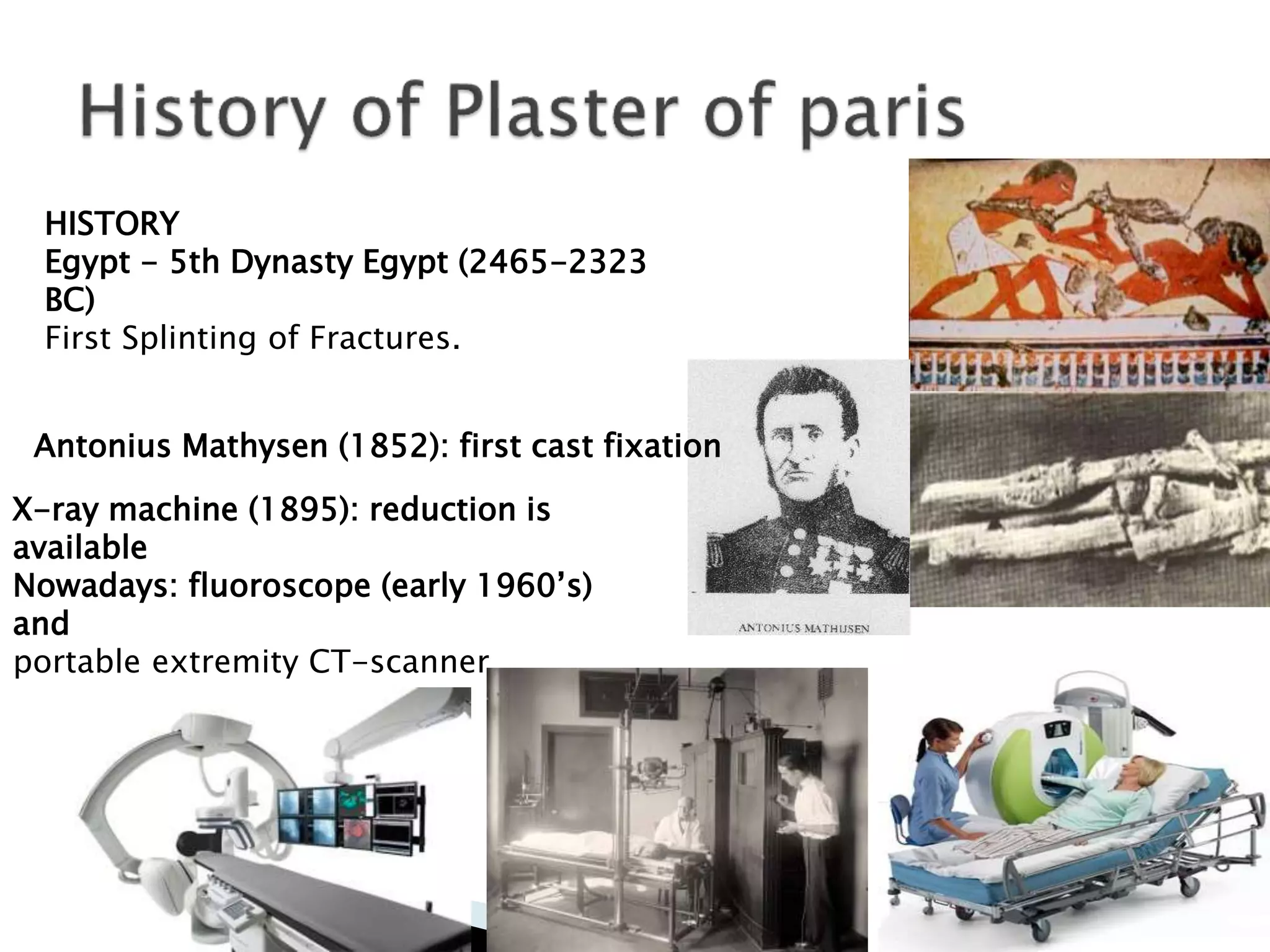
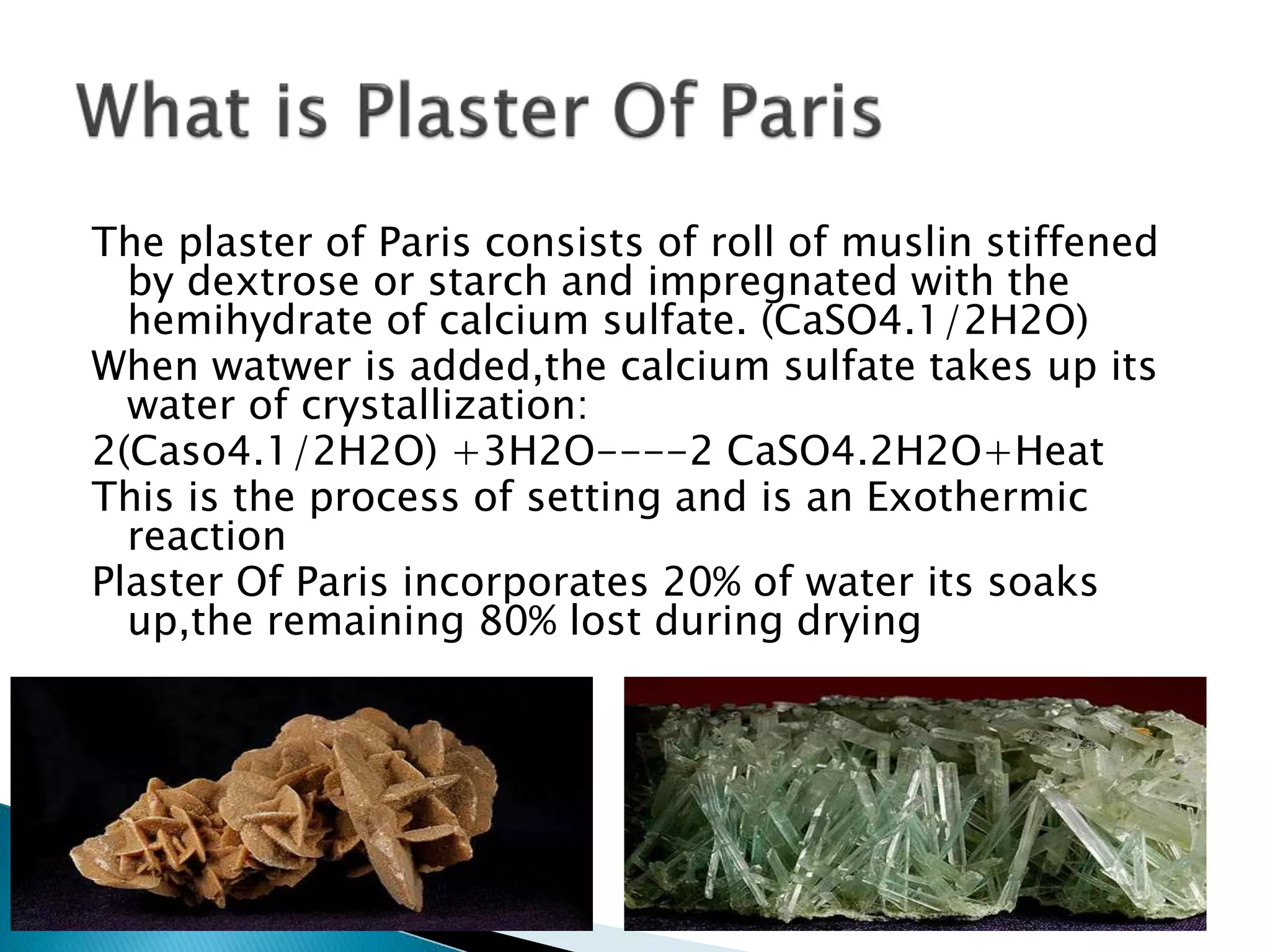
- Plaster of Paris casts were first used in 1852 and set via an exothermic reaction as calcium sulfate rehydrates.
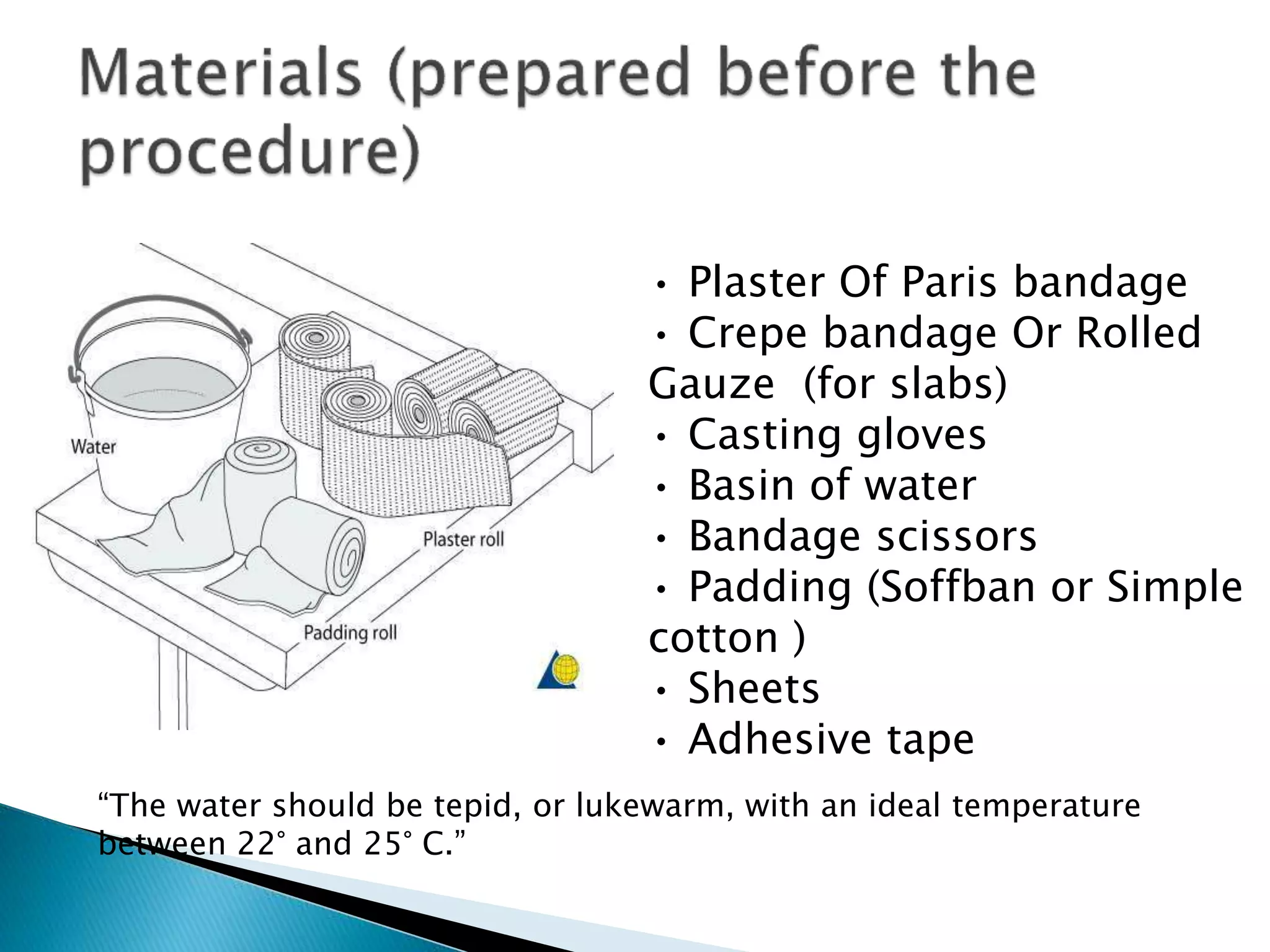
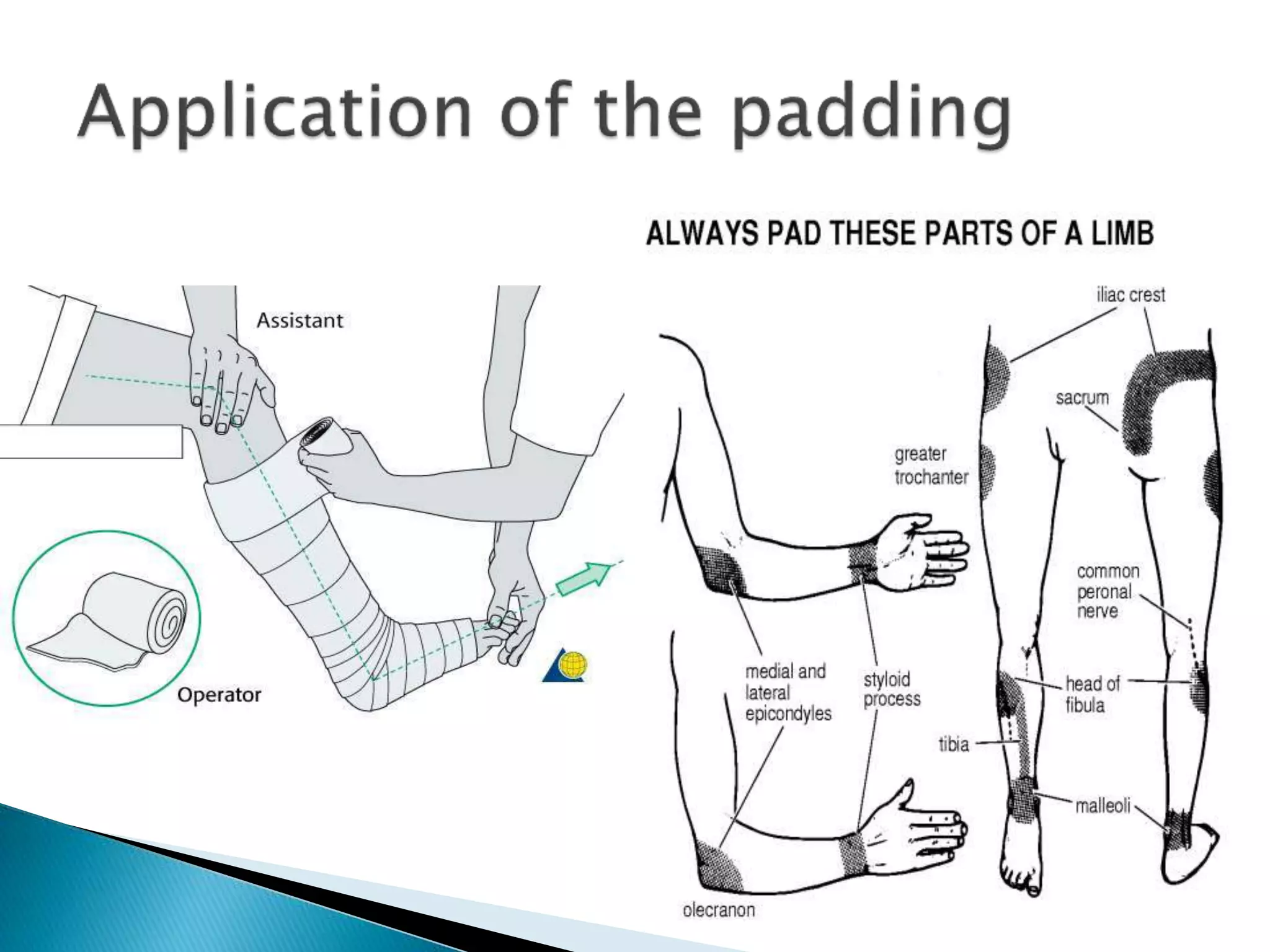
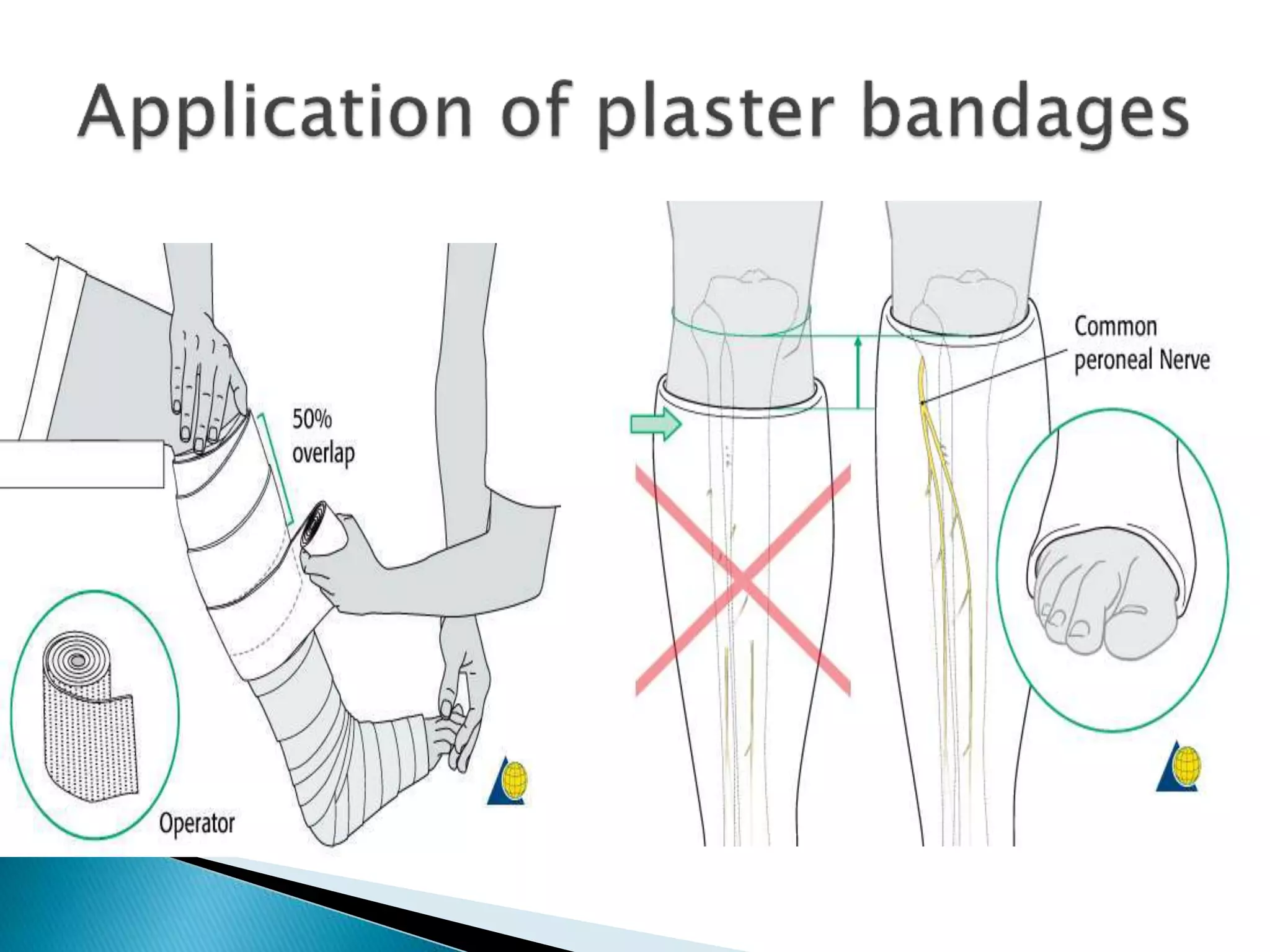
- Proper application involves padding, applying wet plaster in layers with 50% overlap, holding any reductions, and allowing the cast to fully dry.
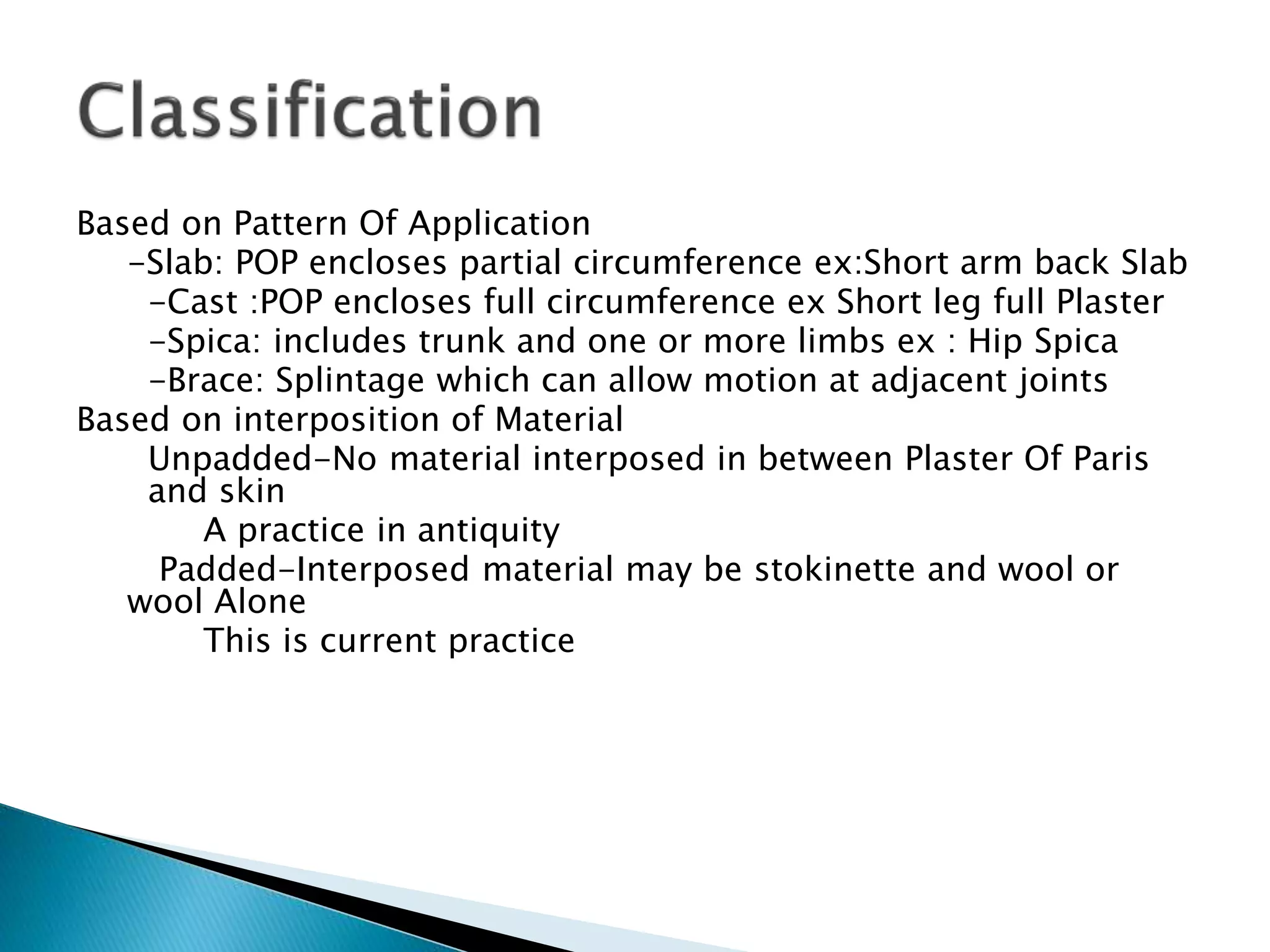
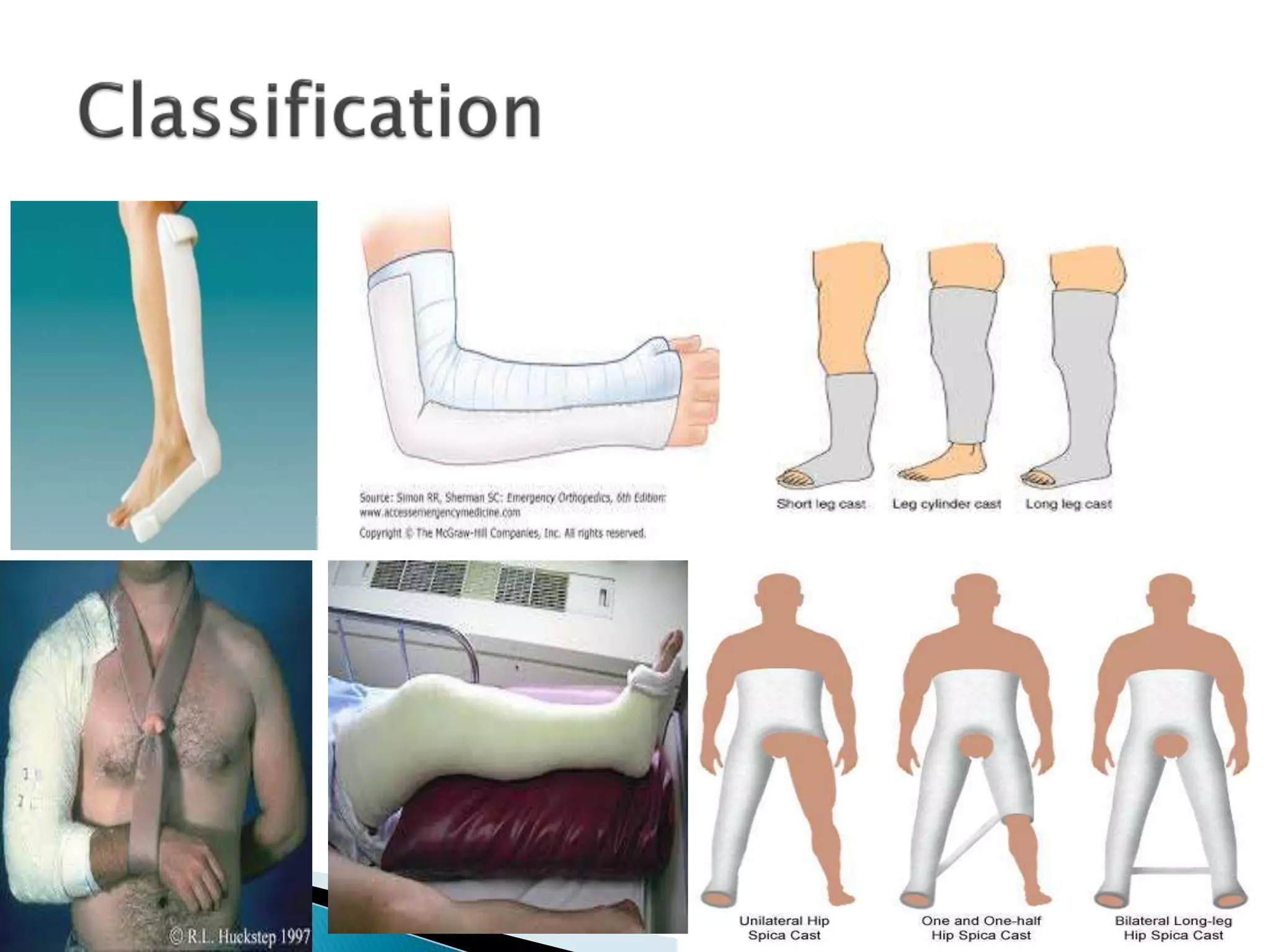
- Common cast types include slabs, full casts, spica casts, and braces. Factors like the fracture and joint positions determine the type.
- Signs of compromised circulation like swelling, numbness, or pain require immediate medical attention. Keeping the cast dry












![ Above Elbow
An above elbow plaster cast or slab is applied
from knuckles of hand (distal palmar crease
anteriorly] and covers lower two thirds of arm
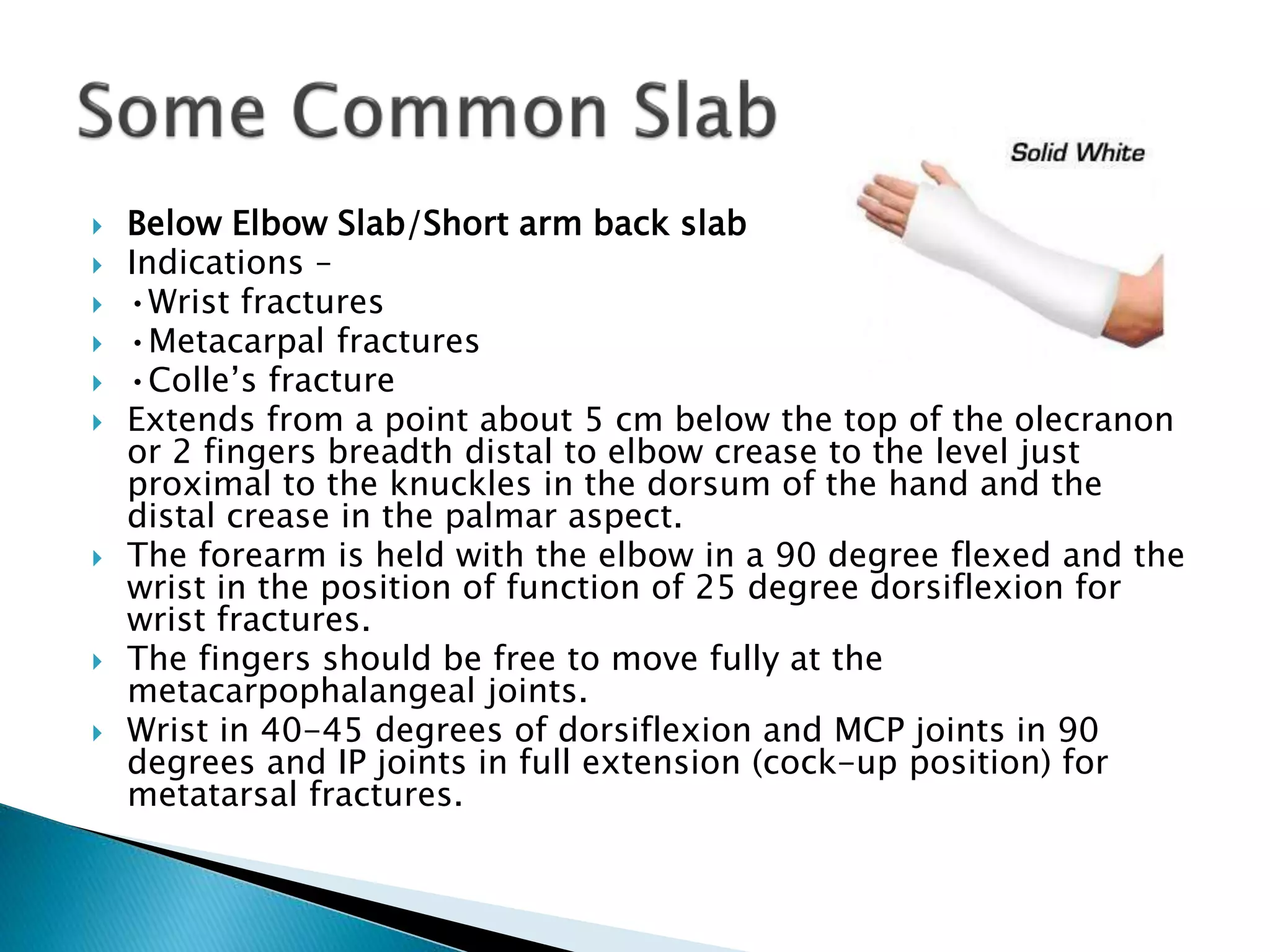
Below Elbow
While distal extent is same as above, proximally
the plaster ends below elbow crease.
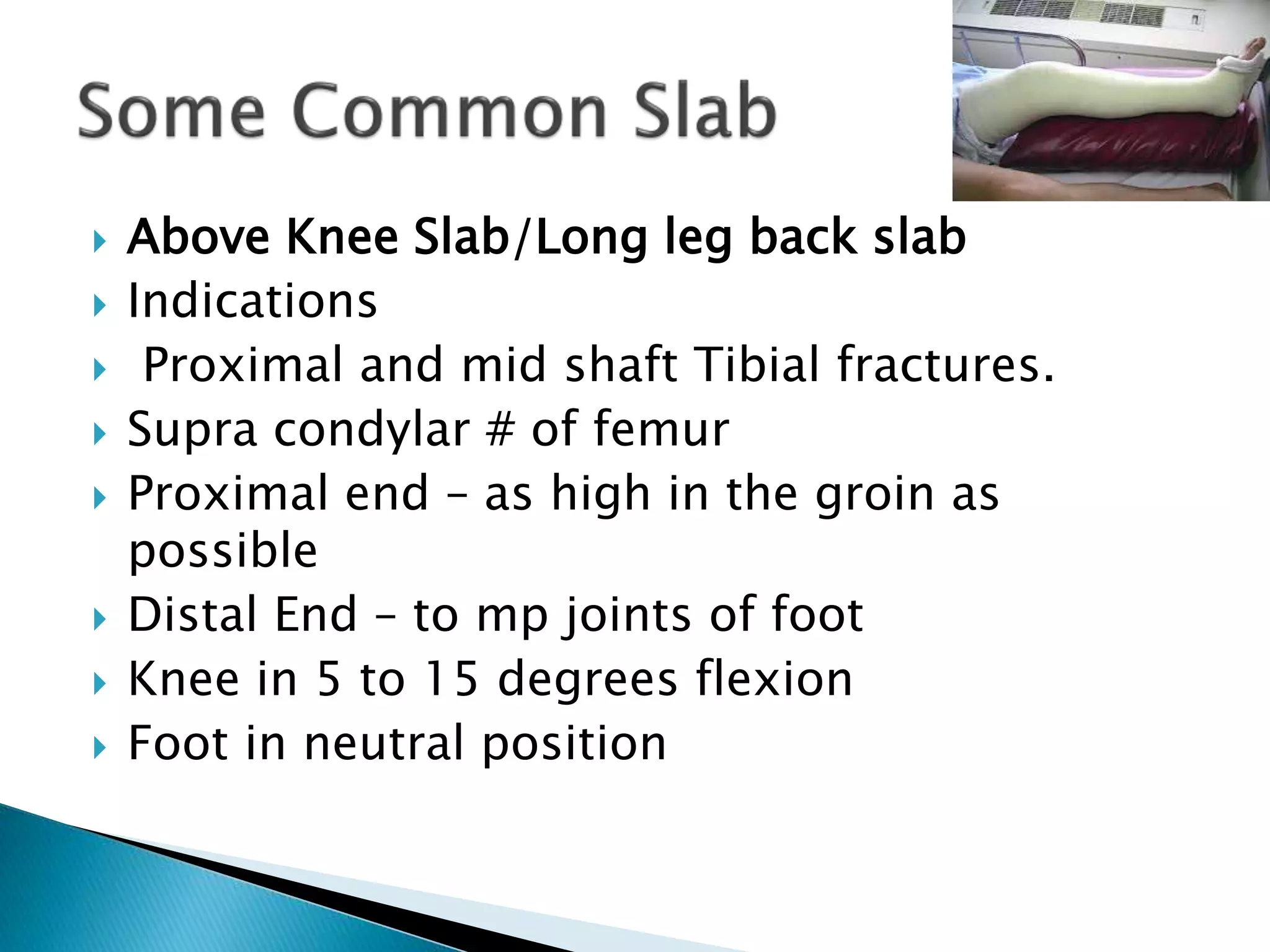
Above Knee
Distal extent is up to metatarsophalangeal joints
and proximally it covers lower two thirds of
thigh.
• Below Knee
Distal extent is same, proximal extent ends below
knee.](https://image.slidesharecdn.com/plasterofparisorthopresentation-180226155821/75/Plaster-of-paris-ortho-presentation-26-2048.jpg)










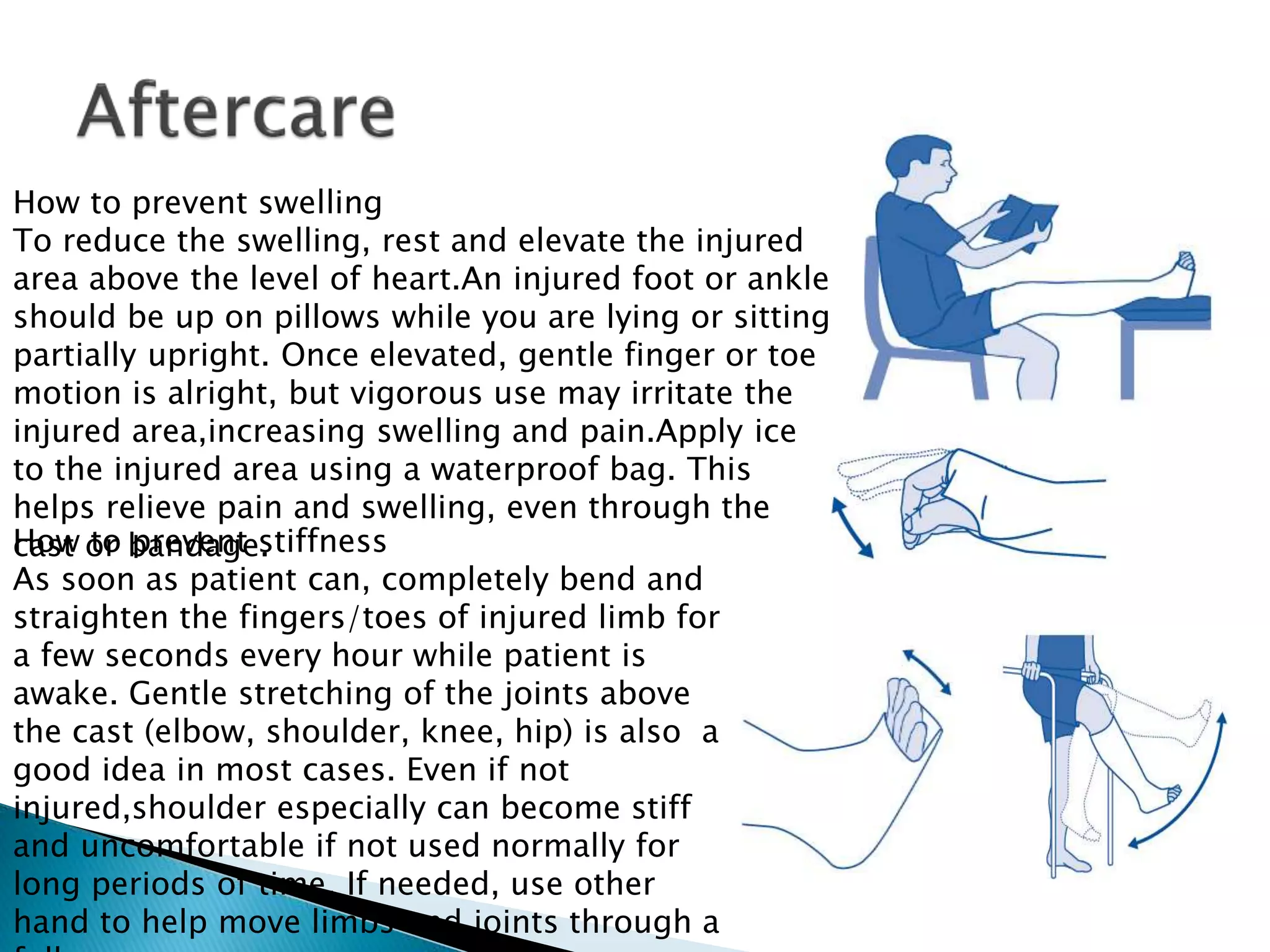













































![Care of bedridden patient [cast]](https://cdn.slidesharecdn.com/ss_thumbnails/careofbedriddenpatientcast-210720163147-thumbnail.jpg?width=640&height=640&fit=bounds)






























