Downloaded 79 times
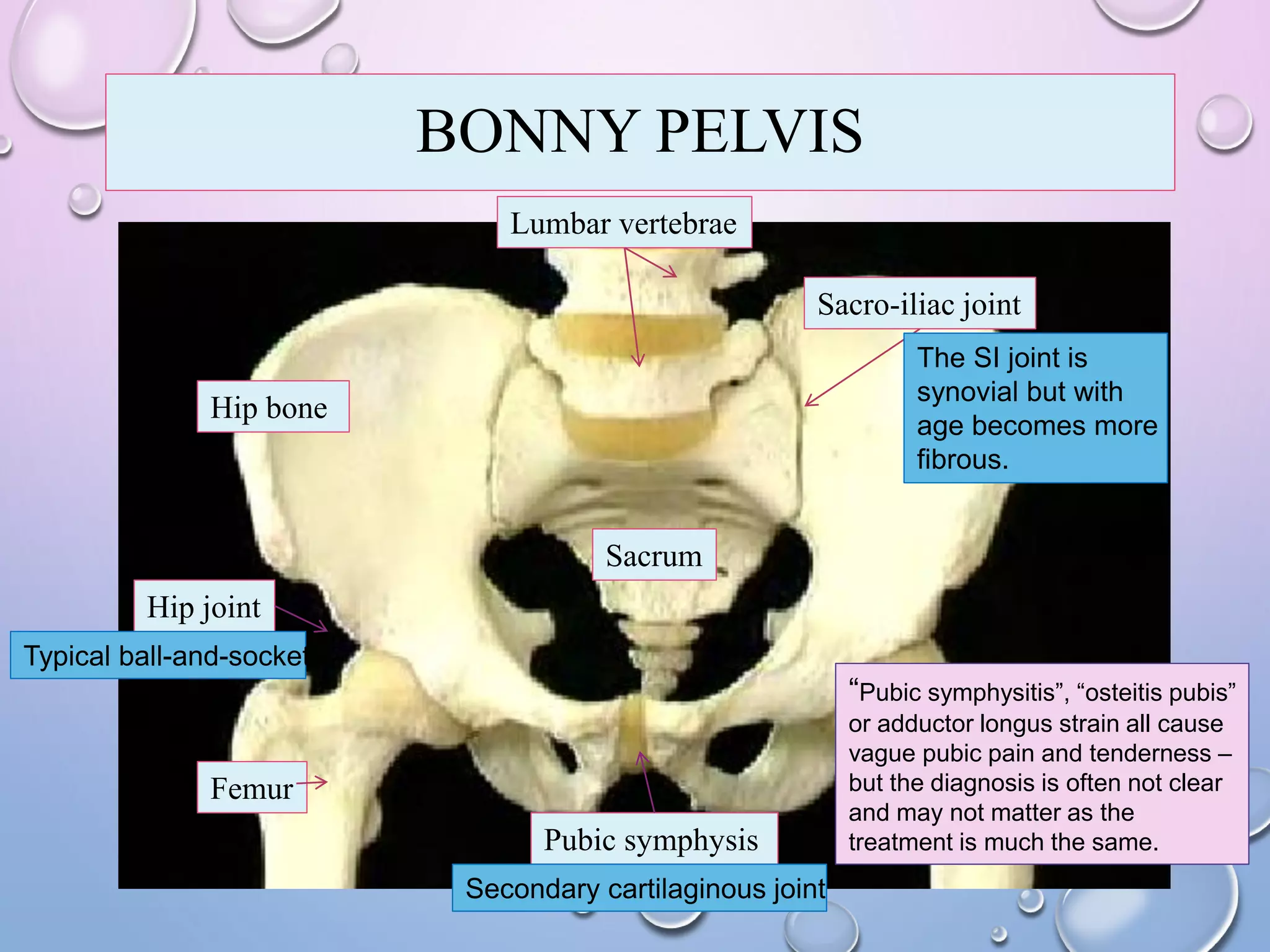














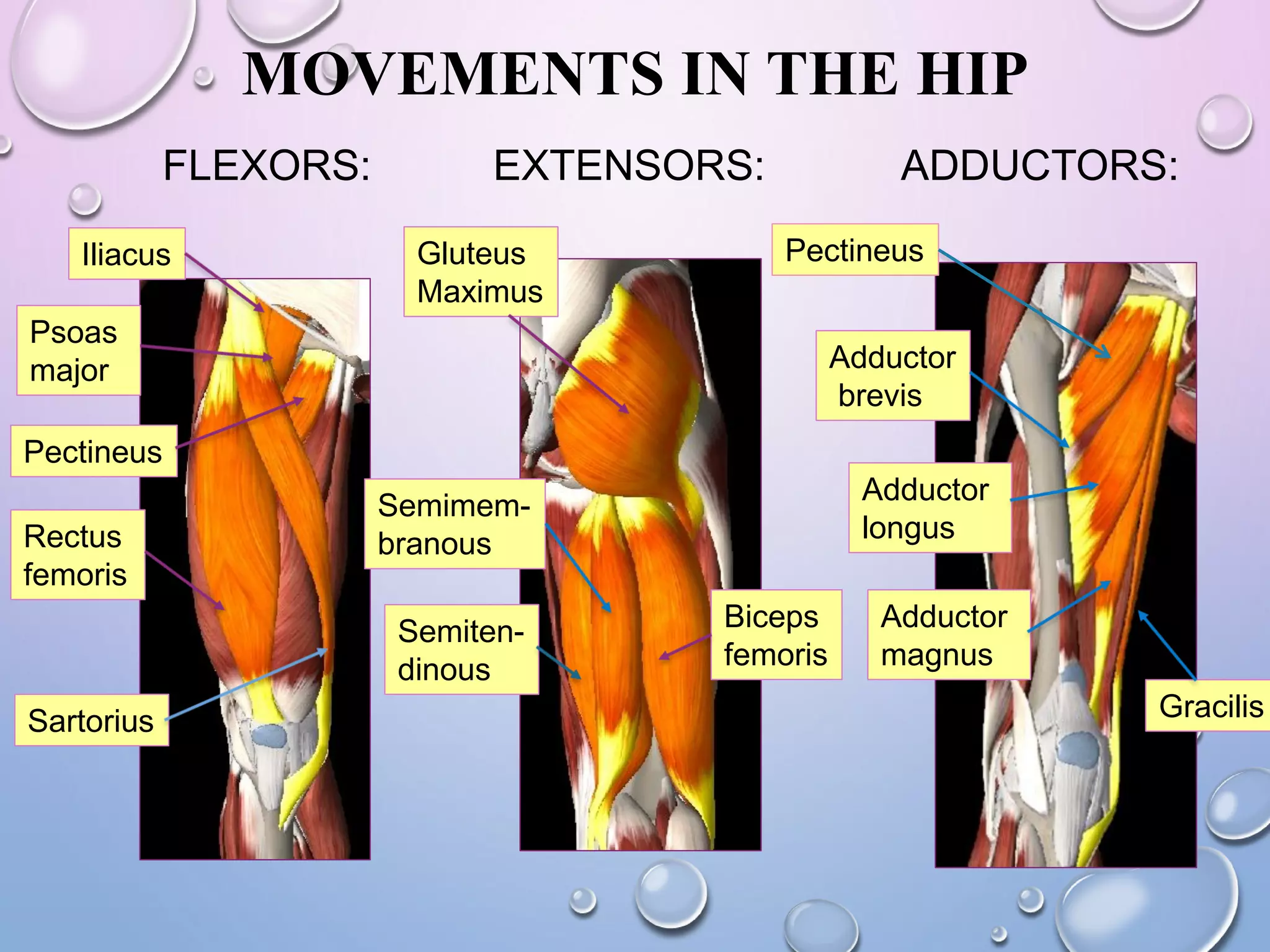











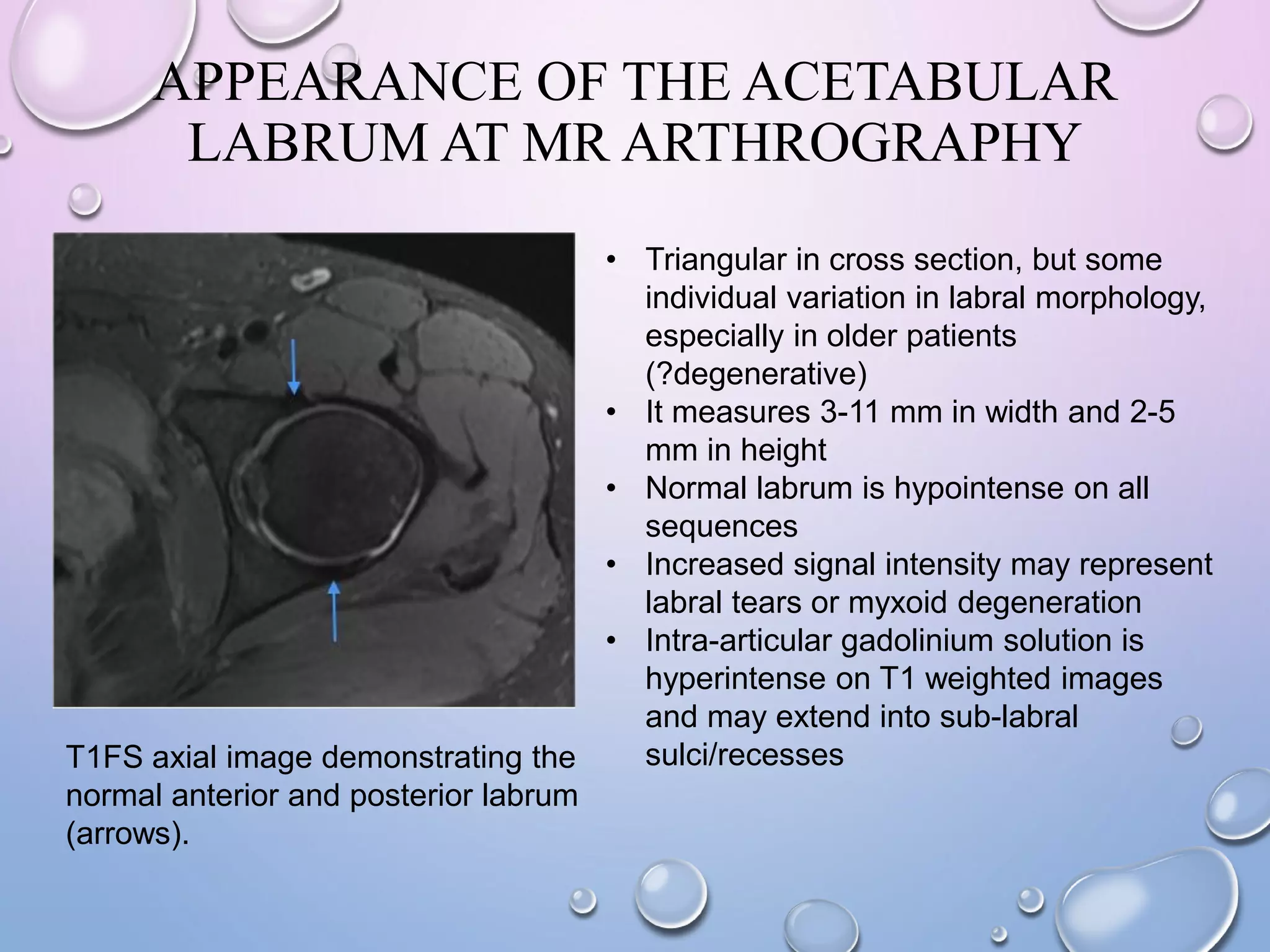




The document provides information on hip anatomy and orthopedic conditions. It discusses: 1) The bones that make up the hip girdle including the hip bone, femur, and sacrum. 2) Joints such as the hip joint and sacroiliac joint. 3) Common hip injuries and conditions like femoral neck fractures, developmental dysplasia of the hip, and labral tears. 4) Imaging appearances of the hip on x-ray, MRI, and MR arthrography that can help identify abnormalities.









































































































