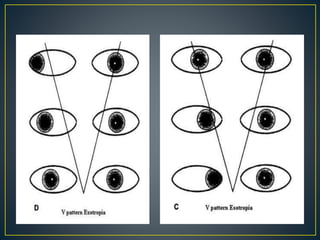
Pattern strabismus occurs when there is a change in the magnitude of horizontal deviation between up and down gaze. The most common types are A pattern (convergence in up gaze) and V pattern (divergence in up gaze). Pattern strabismus can be caused by abnormalities of vertical or horizontal muscle action, anatomical anomalies, disorders of muscle innervation, or anomalous muscle insertions. Evaluation involves measuring the deviation in different gazes using cover-uncover testing and Hess screening. Management may involve adaptation or surgery tailored to the specific pattern, which aims to improve alignment and binocular function.