Downloaded 1,199 times
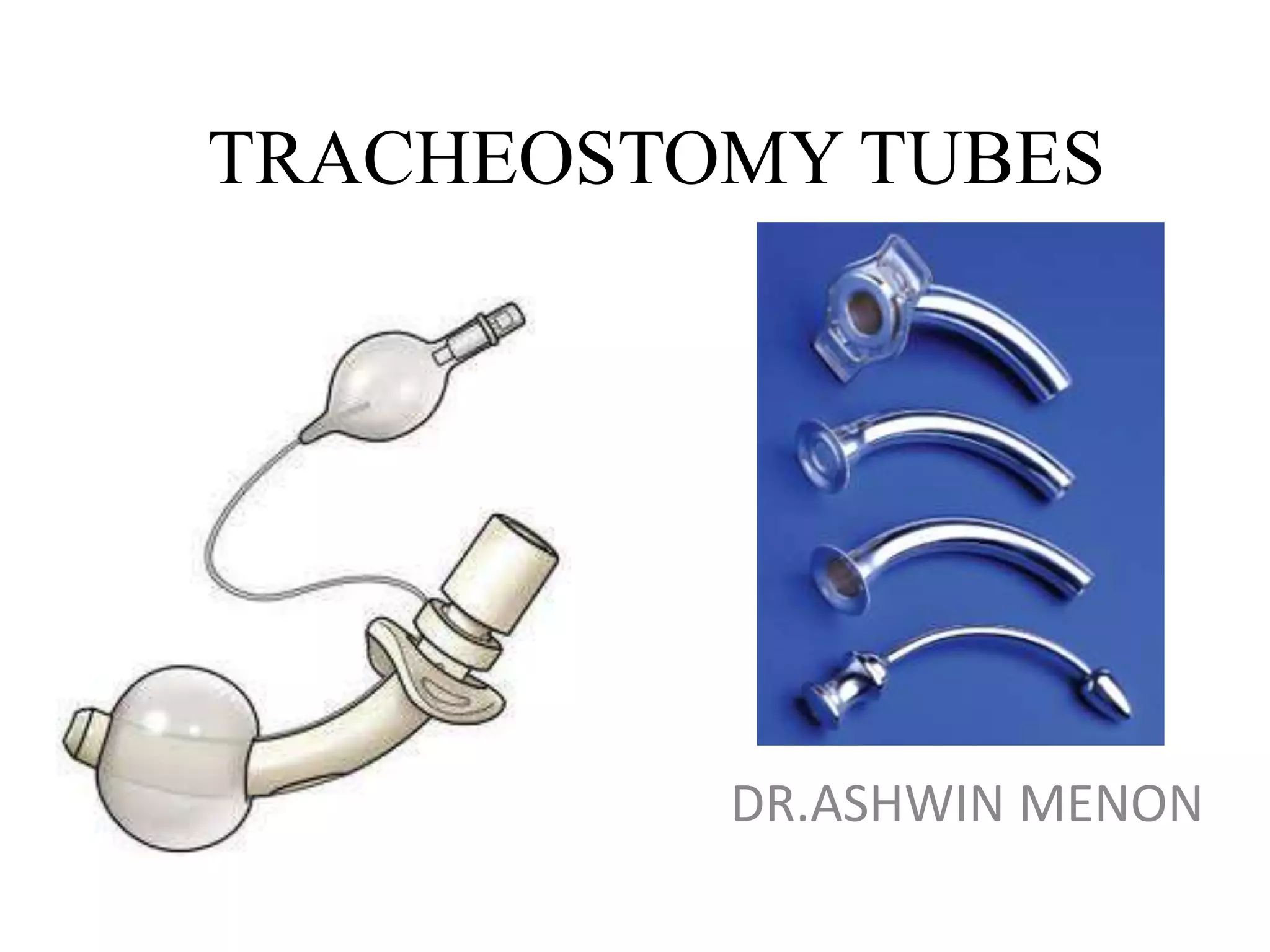
































































This document discusses different types of tracheostomy tubes. It begins by outlining the functions of a tracheostomy tube and describes the ideal properties. It then details the parts of a tracheostomy tube and various types including cuffed, uncuffed, fenestrated, sizes for neonates/pediatrics/adults, and tubes with special features. It provides guidance on selecting the appropriate tube based on a patient's needs and anatomy. Tube accessories like speaking valves and occlusion caps are also described.
































































































