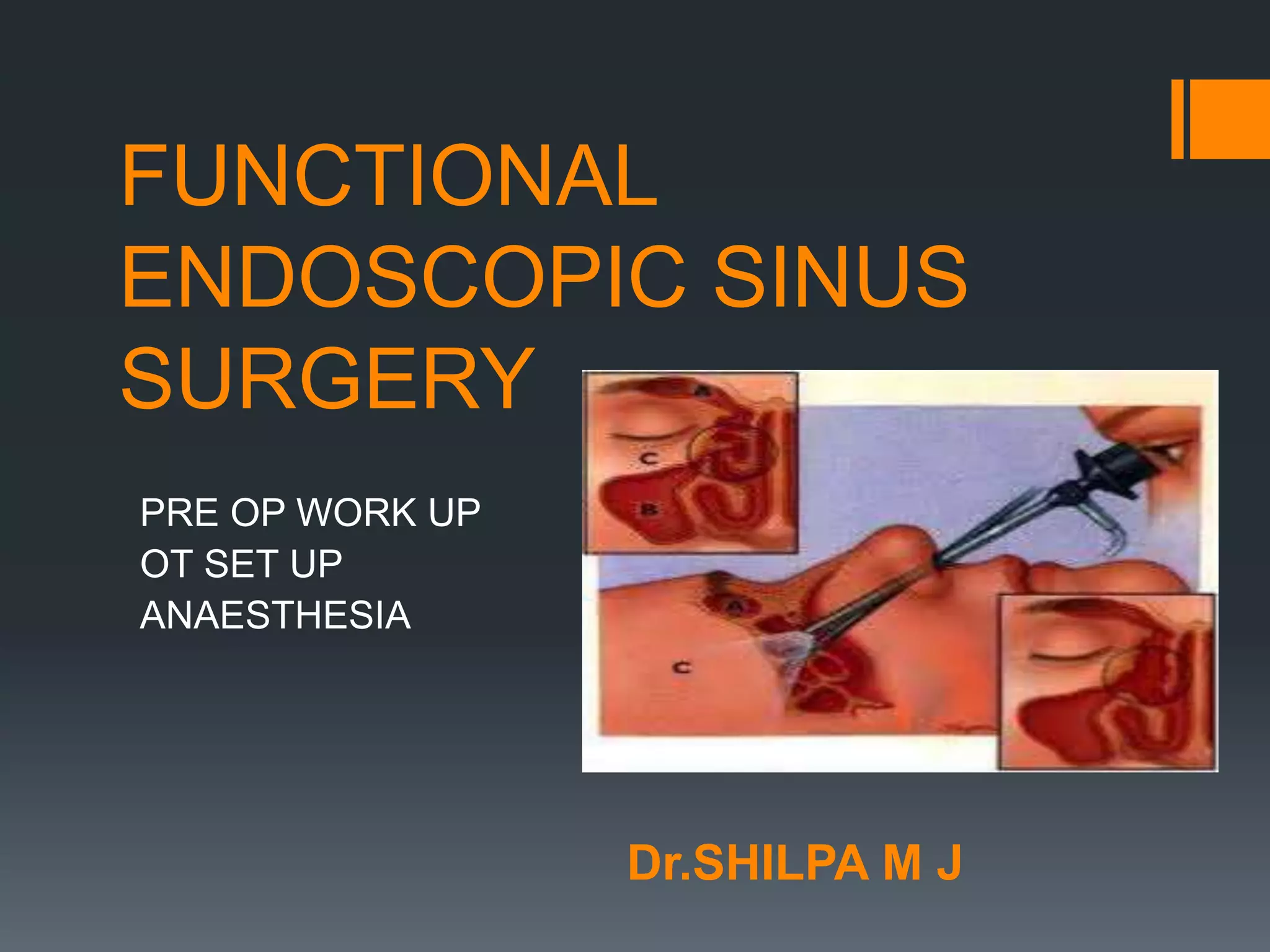
The document outlines the preoperative workup and anesthetic setup for functional endoscopic sinus surgery, detailing essential steps like confirming diagnosis, reviewing medical history, and gathering relevant investigations. It emphasizes the importance of optimizing the patient's preoperative condition, ensuring informed consent, and preparing the operating room with appropriate equipment and instruments. Additionally, it discusses the advantages and disadvantages of both local and general anesthesia in relation to surgical outcomes.