Downloaded 422 times




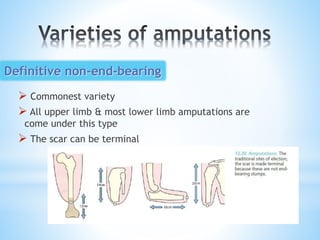
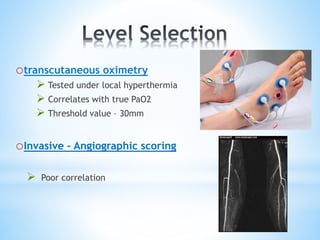
![*Wagner et al (Journal of vascular surgery 1988):
[ clinical judgment is superior to objective
assessments. More distal amputations can
be achieved with clinical measures over objective
studies.]
*Clinical judgment is central to
amputation level selection.](https://image.slidesharecdn.com/amputations-160412094517/85/Amputations-of-extremity-15-320.jpg)





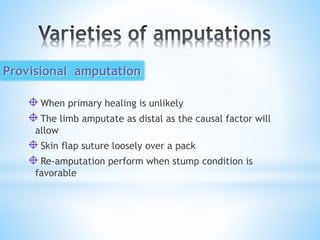
![(Gitter and Bosker 2005):[Yet with appropriate
rehabilitation, many people can learn to walk or
function again and live high quality lives.]
1. Residual Limb Shrinkage and Shaping
2. Limb Desensitization
3. Maintain joint range of motion
4. Strengthen residual limb
5. Maximize Self reliance
6. Patient education: Future goals and prosthetic
options
Rehabilitation](https://image.slidesharecdn.com/amputations-160412094517/85/Amputations-of-extremity-40-320.jpg)

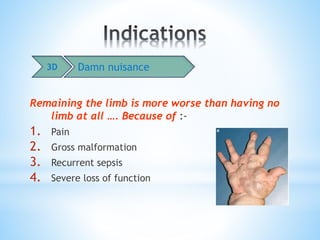
![*Amputation represents loss of
function, sensation and body image.
*(Gitter and Bosker 2005):[Limb loss
is one of the most physically and
psychologically devastating events
that can happen to a person. Not
only does lower limb amputation
cause major disfigurement, it
renders people less mobile and at
risk for loss of independence.]](https://image.slidesharecdn.com/amputations-160412094517/85/Amputations-of-extremity-42-320.jpg)

![• Solomon L., Warwick D. , Nayagam S.,[2010] Apley’s System of Orthopaedics and Fractures, 9th ed.
Hodderarnold comp.,London, UK.
• Miller M. , Thompson S. , Hart J. ,[2012] REVIEW OF ORTHOPAEDICS [PDF], 6th ed. by Saunders, an
imprint of Elsevier Inc. , Philadelphia, USA.
• Canale S. , Beaty J. , [2007] Campbell’s Operative Orthopaedics [PDF], 11th ed. By Mosby, An
Imprint of Elsevier , Tennessee, USA.
• Matthew L., HMO2, [2011] Amputation and Limb Prostheses [PPT]. http://www.authorstream.com/
heier.barb-1256551-amputation2012..ppt (accessed nov. 22, 2011)
• Arvind Lee , [2014] Lower Limb Amputations – Level Selection [PPT]. http://www.austpar.com/
portals/lowerlimbamputationlevelselection.ppt (accessed dec.2003)
• Kovryha M. F., [2010] Basic Surgical Principles of Amputations and Disarticulations of the Upper and
Lower Extremities [PPT]. http://www.slideshare.net/ xatcon/amputation-3286795.ppt.
• Andrew H. Schmidt, David Ring, [2011] Upper Extremity Amputation [PPT].http://www.aota.org/
media/34684/U13_UE_Amputations-tfh-edited.ppt (accessed Feb. 2011)
• Yousaf S., Kieffer W. [ 2013] Management of traumatic amputations at BSUH [PPT]. Brighton and
Sussex medical school . Brighton, UK.
• Der Eingriff . [2000] AMPUTATIONS & PROSTHETICS [E-Book].http://www.thieme.de/amputation/
0000015919440/amputation_prothetics.pdf
• M. Jason Highsmith, [2006] Epidemiology & Statistics associated with Limb Loss & Limb Deficiency
[E-Book]. South Florida , USA. http://www.ncbi.nih.gov/pubmed/21140687/ Epidemiology -
Statistics .pdf
• Wikimedia Foundation, http://www.en.wikipedia.org/wiki/Amputation (last modified Nov, 2015)](https://image.slidesharecdn.com/amputations-160412094517/85/Amputations-of-extremity-45-320.jpg)


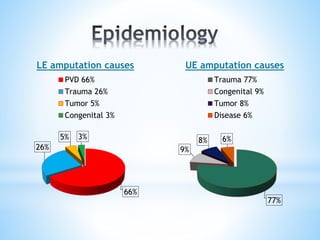
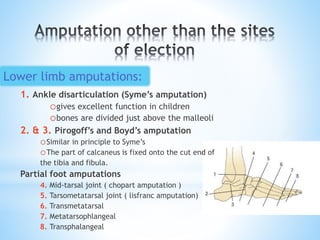
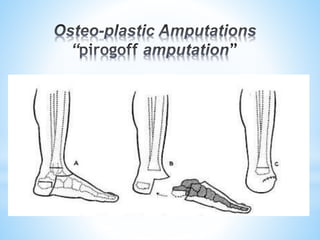
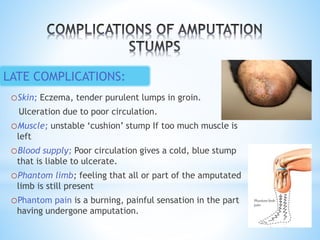
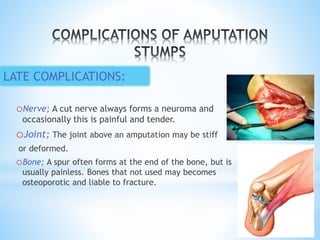
The document discusses the history, procedures, and complications associated with amputation, defining it as the cutting of extremities and detailing its evolution from prehistoric times. It outlines various amputation types, indications for the procedure, and emphasizes the importance of clinical judgment in selecting amputation levels. The text also highlights the psychological and physical impact of limb loss, along with rehabilitation and prosthetic options for amputees.






















































































