LOWER LIMB AMPUTATION Amputation is the surgical removal of a limb or part of a limb, often necessary due to severe injury, infection, or disease, such as cancer or peripheral vascular disease
DR. SHREYA CHAWLA (BPT,MPT ORTHO)
Types of Amputations:
Upper Extremity Amputations: These involve the removal of all or part of an arm, hand, or fingers.
Lower Extremity Amputations: These involve the removal of all or part of a leg, foot, or toes.
Similar to LOWER LIMB AMPUTATION Amputation is the surgical removal of a limb or part of a limb, often necessary due to severe injury, infection, or disease, such as cancer or peripheral vascular disease
LOWER LIMB AMPUTATION Amputation is the surgical removal of a limb or part of a limb, often necessary due to severe injury, infection, or disease, such as cancer or peripheral vascular disease
1.
EVIDENCE BASED
PHYSIOTHERAPY MANAGEMENT
OFLOWER LIMB AMPUTATION
SUBMITTED TO:
DR.MEGHA NIJHAWAN
ASSISTANT PROFESSOR
ISIC(IRS)
SUBMITTED BY:
SHREYA CHAWLA
MPT(MUSCULOSKELETAL)
2nd
YEAR
ISIC(IRS)
2.
INTRODUCTION
Surgical Removal oflimb, partly or totally, from the body, is termed as
Amputation.
Disarticulation is removing the limb through a joint.
More common in men and more often in the lower limb.
3.
Trans:
When the amputationis across the axis of a long bone.
Disarticulation:
When the amputation is between long bones, which anatomically is through the
center of a joint.
Partial:
Amputations of the foot distal to the ankle joint .
Sound Limb
The intact “healthy” limb .
Residual Limb
The extremity of a limb left after amputation, “Stump”
4.
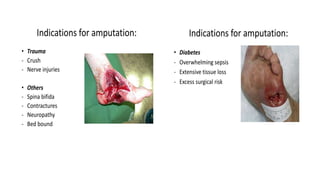
INDICATIONS FOR AMPUTATION
Themajor cause of lower extremity (LE) amputation
Peripheral Vascular Disease (PVD),
Irreversible loss of vascularity to a limb due to diseases
like :
Diabetes,
Berger disease,
Atherosclerosis,
Embolism,
Arterial thrombosis,
Arteriovenous aneurysms or trauma, leading to
gangrene are absolute indications for amputation.
6.
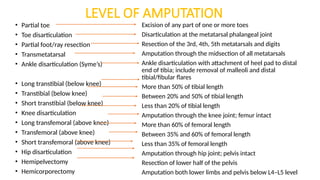
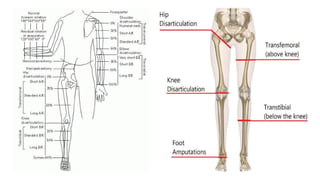
LEVEL OF AMPUTATION
•Partial toe
• Toe disarticulation
• Partial foot/ray resection
• Transmetatarsal
• Ankle disarticulation (Syme’s)
• Long transtibial (below knee)
• Transtibial (below knee)
• Short transtibial (below knee)
• Knee disarticulation
• Long transfemoral (above knee)
• Transfemoral (above knee)
• Short transfemoral (above knee)
• Hip disarticulation
• Hemipelvectomy
• Hemicorporectomy
Excision of any part of one or more toes
Disarticulation at the metatarsal phalangeal joint
Resection of the 3rd, 4th, 5th metatarsals and digits
Amputation through the midsection of all metatarsals
Ankle disarticulation with attachment of heel pad to distal
end of tibia; include removal of malleoli and distal
tibial/fibular flares
More than 50% of tibial length
Between 20% and 50% of tibial length
Less than 20% of tibial length
Amputation through the knee joint; femur intact
More than 60% of femoral length
Between 35% and 60% of femoral length
Less than 35% of femoral length
Amputation through hip joint; pelvis intact
Resection of lower half of the pelvis
Amputation both lower limbs and pelvis below L4–L5 level
Hip Disarticulation
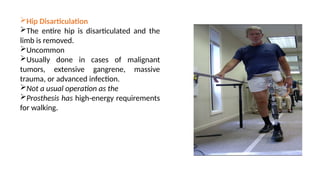
The entirehip is disarticulated and the
limb is removed.
Uncommon
Usually done in cases of malignant
tumors, extensive gangrene, massive
trauma, or advanced infection.
Not a usual operation as the
Prosthesis has high-energy requirements
for walking.
10.
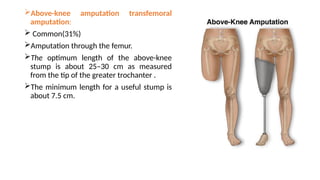
Above-knee amputation transfemoral
amputation:
Common(31%)
Amputation through the femur.
The optimum length of the above-knee
stump is about 25–30 cm as measured
from the tip of the greater trochanter .
The minimum length for a useful stump is
about 7.5 cm.
11.
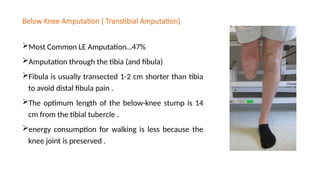
Below Knee Amputation( Transtibial Amputation)
Most Common LE Amputation…47%
Amputation through the tibia (and fibula)
Fibula is usually transected 1-2 cm shorter than tibia
to avoid distal fibula pain .
The optimum length of the below-knee stump is 14
cm from the tibial tubercle .
energy consumption for walking is less because the
knee joint is preserved .
12.
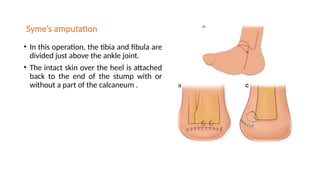
Syme’s amputation
• Inthis operation, the tibia and fibula are
divided just above the ankle joint.
• The intact skin over the heel is attached
back to the end of the stump with or
without a part of the calcaneum .
13.
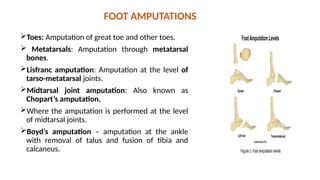
FOOT AMPUTATIONS
Toes: Amputationof great toe and other toes.
Metatarsals: Amputation through metatarsal
bones.
Lisfranc amputation: Amputation at the level of
tarso-metatarsal joints.
Midtarsal joint amputation: Also known as
Chopart’s amputation,
Where the amputation is performed at the level
of midtarsal joints.
Boyd’s amputation – amputation at the ankle
with removal of talus and fusion of tibia and
calcaneus.
14.
TYPES OF AMPUTATION
CLOSEDAMPUTATION
• In this type of
amputation, the stump is
closed primarily over the
bony stump by retaining
skin and muscles at least
5 cm distal to the bone
end to facilitate closing
of the stump.
OPEN AMPUTATION
• It is undertaken as an
emergency procedure
and is also called
guillotine amputation.
• In this type of
amputation, the skin is
not closed over the
amputation stump .
• The stump is then
covered by skin grafting
or secondary closure
15.
SURGICAL PRINCIPLES
• Thereare two surgical procedures to managing the muscles during amputation:
myodesis and myoplasty.
• In myodesis , the muscles and fasciae are sutured directly to the distal residual bone
through drill holes. The muscles inserted function better, resulting in good prosthetic
control. The procedure compromises blood supply to the muscles and hence is
contraindicated in patients with severe peripheral vascular disease. Sometimes
myodesis fails even with the best of care.
• Myoplasty, on the other hand, requires the surgeon to suture the opposing muscles in
the residual limb to each other and to the periosteum or to the distal end of the cut
bone. The muscles must be stretched just enough so that they control the residual limb.
The muscles sutured to each other provide distal soft-tissue padding over the residual
bone. Sometimes a painful bursa develops between the soft tissues and the underlying
bone. Some of these bursae can become infected and painful.
16.
• Some ofthe principles of surgery are:
• The use of a tourniquet is advised to obtain a bloodless field—except in ischemic
conditions.
• Level of amputation—efforts should be made to preserve all possible limb length,
keeping in mind the prosthesis to be fit.
• Skin flaps—skin should be mobile, sensation intact, and with no adherent scars.
• Muscles are divided 3 to 5 cm distal to the level of bone resection.
• Nerves are gently pulled and cut cleanly so that they retract well proximal to the
bone level. This reduces the complication of a neuroma.
17.
Complication of amputation
Failureof healing due either to wrong shaping of the flaps or inadequate blood
supply.
Recurrence of the disease, infection or neoplasm for which the amputation was
performed.
• Painful neuroma.
• Phantom limb pain.
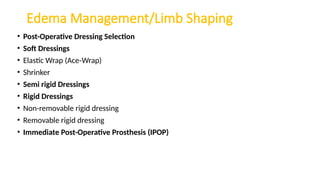
Elastic Wrap
• Advantages
•Can assist in shaping limb
• Low cost
• Wound accessibility
• Easy to apply with some patients
• Can be washed .
• Disadvantages
• Must be reapplied every 2 hours for
edema control
• Can be difficult to apply
• Can slip off limb with exercise or
mobility
21.
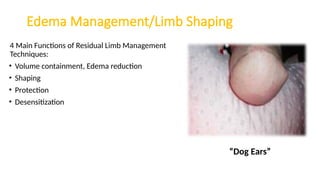
Shrinker
Advantages
• Can beeasily applied.
• Wound accessibility.
• Graded pressure (high to low) from distal to proximal.
Disadvantages
• May cause incision dehiscence if applied improperly
• May be too painful to apply and wear immediately post-
op
PHASES OF CARE:
POSTSURGICALAND PREPROSTHETIC
• The rehabilitation program can be arbitrarily divided into two phases:
(1) The postsurgical phase is the time between surgery and discharge from the hospital
(2) The preprosthetic phase runs from hospital discharge to prosthetic fitting or a decision
that the patient is not a candidate for prosthetic fitting.
25.
Early Postsurgical Evaluation
•General systems review
• Postsurgical status
Cardiovascular
Respiratory
Diabetes control (if appropriate)
Whether out of bed
Infection?
• Pain
Incisional
Phantom
Other
• Vascularity (if appropriate)
• Functional status
Bed mobility, transfers, sitting,
standing, balance
• Gross range of motion
Unamputated extremity
Hip, knee flexion and extension
Ankle dorsiflexion/plantarflexion
• Upper extremity to note any
limitations that would interfere with
functional activities
• Amputated extremity
26.
Postsurgical Phase
Immediate PostSurgical Phase
Goals
Ensure medical stability
Promote wound healing
Reduce edema
Prevent loss of motion
Increase UE and LE strength
Promote mobility and self-care
Promote sound limb care
Assist with limb loss adjustment
EDUCATE, EDUCATE, EDUCATE!
27.
Patient education
• Themore the patient and family understand about the amputation and
rehabilitation process the better the outcome.
• Understand the need for continued care, and become active participation in the
rehabilitation program.
• home program need to be developed.
• Encouraged to be as mobile as possible.
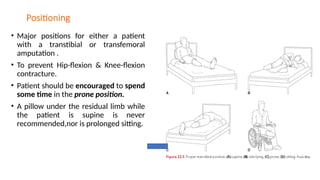
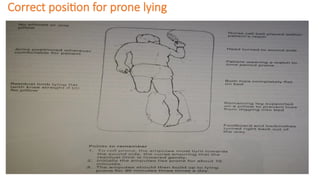
Positioning
• Major positionsfor either a patient
with a transtibial or transfemoral
amputation .
• To prevent Hip-flexion & Knee-flexion
contracture.
• Patient should be encouraged to spend
some time in the prone position.
• A pillow under the residual limb while
the patient is supine is never
recommended,nor is prolonged sitting.
Mobility
Teach the patientsafe and independent mobility with crutches is much more
beneficial.
While there is more stability in a walker, there is greater flexibility in
accomplishing (ADL) on crutches.
If the patient has been fitted with an IPOP or an RRD and has good control of
weight-bearing,
Might decide to add a pylon and foot to the assembly making partial weight-
bearing gait possible.
When teaching mobility to someone with diabetes or any vascular
compromise, it is critical that the patient wear a shoe on the remaining foot.
33.
Balance and Transfers
Standingbalance exercises on the remaining extremity can be quite beneficial in
helping the individual regain a sense of his or her body in space .
In the early postsurgical period the person should stand and transfer leading with
the unamputated limb to protect the residual limb from possible injury against the
chair or bed.
34.
Sound Limb Care
DailySkin Inspection
Systematic Inspections
Attention to bony prominences
Attention to problem areas
Ensure patient can see feet .
Skin Cleansing
Routine on a daily basis,
Avoid hot water
Use mild cleaning agents, Avoid
perfumed soaps
Minimize skin exposure to excessive
moisture (Perspiration, Wet weather,
Wound drainage, Incontinence)
However maintain adequate moisture
(Reduce friction,Hydrate skin, Maintains
tissue elasticity).
Footwear
NEVER walk barefoot
Dry Cotton or Wool Socks, White Preferred
Extra Depth or Custom Shoes…Need
support!
Inspect shoes for tacks, nails, rocks.
35.
Residual Limb Care
ThePhysical Therapist will need to teach the patient and family how to
properly wrap tha limb.
The patient should not put pressure on the limb or drag it on the bed.
Slightly raising the residual limb and moving it to the side while rolling to the
unamputated side is the best way to come to the sitting.
Move the limb in pain free range
Gentle hip extension is the best exercise to teach the patient while lying on
the unamputated side. (several times a day)
Avoid resistive exercise for the residual limb.
36.
Preprosthetic phase
• Thepreprosthetic phase runs from hospital discharge to prosthetic fitting or a
decision that the patient is not a candidate for prosthetic fitting.
39.
Pre-Prosthetic Training Phase
•The preprosthetic phase is the time between discharge from the acute care
hospital and fitting with a definitive prosthesis, or the decision not to fit the
patient with an artificial limb.
40.
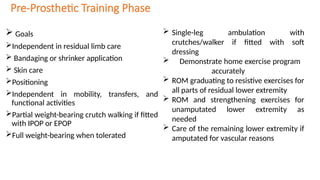
Pre-Prosthetic Training Phase
Goals
Independent in residual limb care
Bandaging or shrinker application
Skin care
Positioning
Independent in mobility, transfers, and
functional activities
Partial weight-bearing crutch walking if fitted
with IPOP or EPOP
Full weight-bearing when tolerated
Single-leg ambulation with
crutches/walker if fitted with soft
dressing
Demonstrate home exercise program
accurately
ROM graduating to resistive exercises for
all parts of residual lower extremity
ROM and strengthening exercises for
unamputated lower extremity as
needed
Care of the remaining lower extremity if
amputated for vascular reasons
41.
Intervention
Residual Limb care
Residuallimb wrapping
Patients tend to wrap their own residual limb in a circular manner, often creating a
tourniquet, which may compromise healing and faster the development of a
bulbous end. Although the transtibial residual limb can be effectively wrapped in a
sitting position, it is difficult to properly wrap and anchor the transfemoral limb
while sitting.
42.
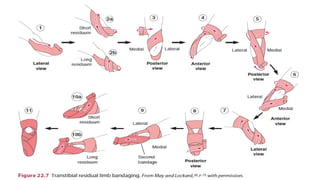
The Transtibial Bandage
Two4-in elastic bandages are usually
enough to wrap most transtibial residual
limbs.
Very large residual limbs may require
three bandages.
Care should be taken to completely
cover the residual limb with a firm and
even pressure.
Each turn should partially overlap other
turns so the whole residual limb is well
covered.
The pattern is usually from proximal to distal
and back to proximal, starting at the tibial
condyles and covering both condyles
Usually, the patella is left free to aid in knee
motion, although with extremely short
residual limbs, it may be necessary to cover it
for better suspension.
The second bandage is wrapped like the first,
except that it is started at the opposite tibial
condyle from the first bandage .
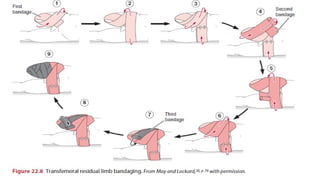
45.
The Transfemoral Bandage
Thepreferred method of wrapping the transfemoral residual limb with the task
being doneby a family member or caregiver.
The side-lying position is preferred for better control of the residual limb with the
hip neutral or slightly extended.
Wrapping the transfemoral residual limb in the sitting position is difficult and
usually leaves an area on the medial thigh uncovered.
For most residual limbs, two 6-in bandages
47.
Skin care
• Properhygiene and skin care are important.
• Kept clean and dry , use skin lotions.
• Care must be taken to avoid abrasions, cut, and other skin problem.
48.
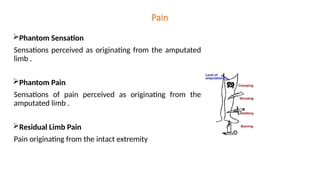
Pain
Phantom Sensation
Sensations perceivedas originating from the amputated
limb .
Phantom Pain
Sensations of pain perceived as originating from the
amputated limb .
Residual Limb Pain
Pain originating from the intact extremity
49.
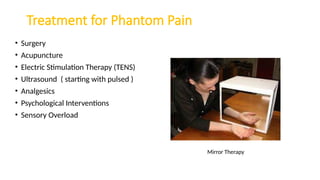
Treatment for PhantomPain
• Surgery
• Acupuncture
• Electric Stimulation Therapy (TENS)
• Ultrasound ( starting with pulsed )
• Analgesics
• Psychological Interventions
• Sensory Overload
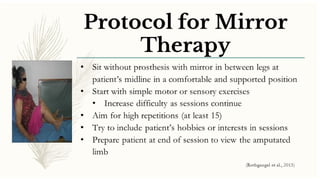
Mirror Therapy
51.
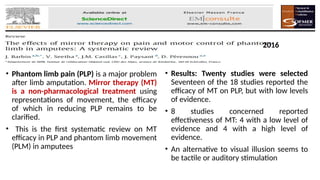
• Phantom limbpain (PLP) is a major problem
after limb amputation. Mirror therapy (MT)
is a non-pharmacological treatment using
representations of movement, the efficacy
of which in reducing PLP remains to be
clarified.
• This is the first systematic review on MT
efficacy in PLP and phantom limb movement
(PLM) in amputees
• Results: Twenty studies were selected
Seventeen of the 18 studies reported the
efficacy of MT on PLP, but with low levels
of evidence.
• 8 studies concerned reported
effectiveness of MT: 4 with a low level of
evidence and 4 with a high level of
evidence.
• An alternative to visual illusion seems to
be tactile or auditory stimulation
2016
52.
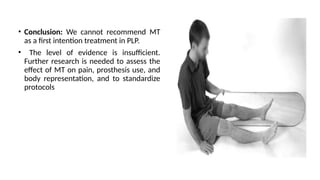
• Conclusion: Wecannot recommend MT
as a first intention treatment in PLP.
• The level of evidence is insufficient.
Further research is needed to assess the
effect of MT on pain, prosthesis use, and
body representation, and to standardize
protocols
53.
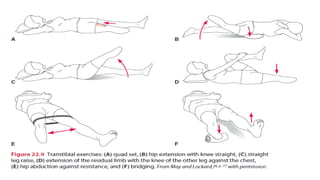
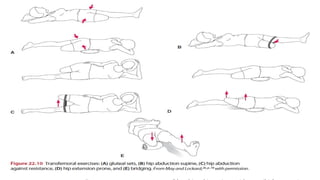
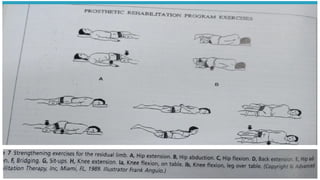
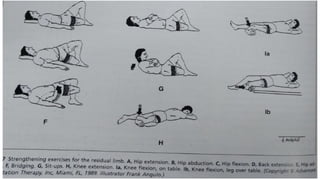
Exercises
• The exerciseprogram is individually designed and includes strengthening, balance, and coordination
activities.
• The type of postsurgical dressing, degree of postoperative pain, and healing of the incision will
determine when resistive exercises for the involved extremity can be started.
• The exercise program can take many forms and must include a home exercise program (HEP).
• The hip extensors and abductors and knee extensors and flexors are particularly important for
prosthetic ambulation.
• Studies have shown a correlation between strength of the key muscle groups and ability to use a
prosthesis effectively.
• Figures 22.9 and 22.10 depict a series of exercises particularly well designed to strengthen key
muscles around the hip and knee.
• These exercises can be adapted for a HEP because they are simple to perform and require no special
equipment.
• Exercises need to be progressed with increased resistance.
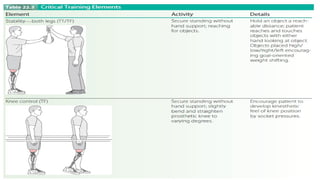
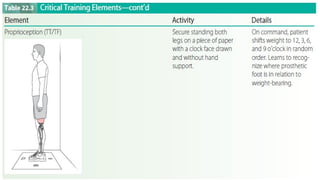
58.
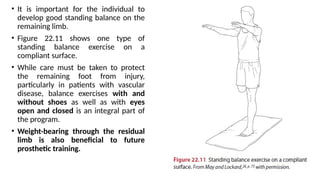
• It isimportant for the individual to
develop good standing balance on the
remaining limb.
• Figure 22.11 shows one type of
standing balance exercise on a
compliant surface.
• While care must be taken to protect
the remaining foot from injury,
particularly in patients with vascular
disease, balance exercises with and
without shoes as well as with eyes
open and closed is an integral part of
the program.
• Weight-bearing through the residual
limb is also beneficial to future
prosthetic training.
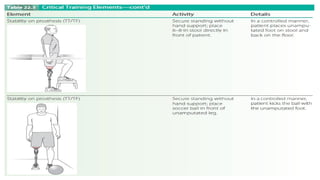
59.
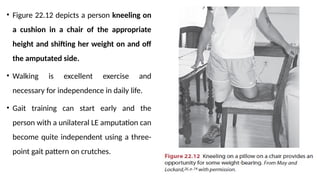
• Figure 22.12depicts a person kneeling on
a cushion in a chair of the appropriate
height and shifting her weight on and off
the amputated side.
• Walking is excellent exercise and
necessary for independence in daily life.
• Gait training can start early and the
person with a unilateral LE amputation can
become quite independent using a three-
point gait pattern on crutches.
60.
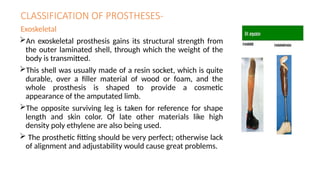
CLASSIFICATION OF PROSTHESES-
Exoskeletal
Anexoskeletal prosthesis gains its structural strength from
the outer laminated shell, through which the weight of the
body is transmitted.
This shell was usually made of a resin socket, which is quite
durable, over a filler material of wood or foam, and the
whole prosthesis is shaped to provide a cosmetic
appearance of the amputated limb.
The opposite surviving leg is taken for reference for shape
length and skin color. Of late other materials like high
density poly ethylene are also being used.
The prosthetic fitting should be very perfect; otherwise lack
of alignment and adjustability would cause great problems.
61.
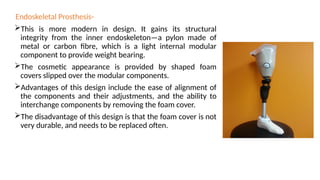
Endoskeletal Prosthesis-
This ismore modern in design. It gains its structural
integrity from the inner endoskeleton—a pylon made of
metal or carbon fibre, which is a light internal modular
component to provide weight bearing.
The cosmetic appearance is provided by shaped foam
covers slipped over the modular components.
Advantages of this design include the ease of alignment of
the components and their adjustments, and the ability to
interchange components by removing the foam cover.
The disadvantage of this design is that the foam cover is not
very durable, and needs to be replaced often.
62.
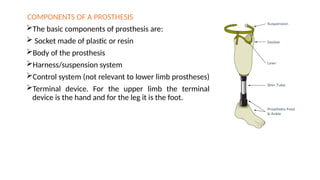
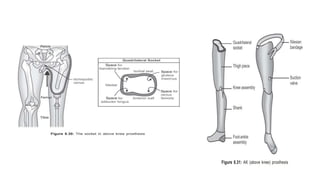
COMPONENTS OF APROSTHESIS
The basic components of prosthesis are:
Socket made of plastic or resin
Body of the prosthesis
Harness/suspension system
Control system (not relevant to lower limb prostheses)
Terminal device. For the upper limb the terminal
device is the hand and for the leg it is the foot.
63.
PROSTHESIS FOR THELOWER EXTREMITY
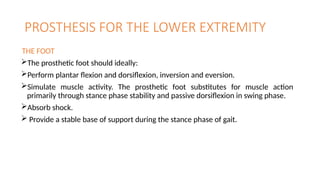
THE FOOT
The prosthetic foot should ideally:
Perform plantar flexion and dorsiflexion, inversion and eversion.
Simulate muscle activity. The prosthetic foot substitutes for muscle action
primarily through stance phase stability and passive dorsiflexion in swing phase.
Absorb shock.
Provide a stable base of support during the stance phase of gait.
64.
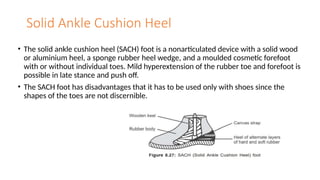
Solid Ankle CushionHeel
• The solid ankle cushion heel (SACH) foot is a nonarticulated device with a solid wood
or aluminium heel, a sponge rubber heel wedge, and a moulded cosmetic forefoot
with or without individual toes. Mild hyperextension of the rubber toe and forefoot is
possible in late stance and push off.
• The SACH foot has disadvantages that it has to be used only with shoes since the
shapes of the toes are not discernible.
65.
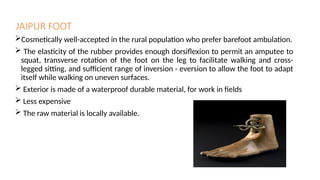
JAIPUR FOOT
Cosmetically well-acceptedin the rural population who prefer barefoot ambulation.
The elasticity of the rubber provides enough dorsiflexion to permit an amputee to
squat, transverse rotation of the foot on the leg to facilitate walking and cross-
legged sitting, and sufficient range of inversion - eversion to allow the foot to adapt
itself while walking on uneven surfaces.
Exterior is made of a waterproof durable material, for work in fields
Less expensive
The raw material is locally available.
66.
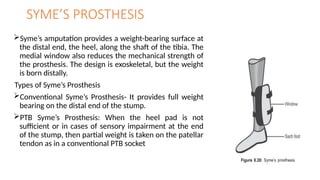
SYME’S PROSTHESIS
Syme’s amputationprovides a weight-bearing surface at
the distal end, the heel, along the shaft of the tibia. The
medial window also reduces the mechanical strength of
the prosthesis. The design is exoskeletal, but the weight
is born distally.
Types of Syme’s Prosthesis
Conventional Syme’s Prosthesis- It provides full weight
bearing on the distal end of the stump.
PTB Syme’s Prosthesis: When the heel pad is not
sufficient or in cases of sensory impairment at the end
of the stump, then partial weight is taken on the patellar
tendon as in a conventional PTB socket
67.
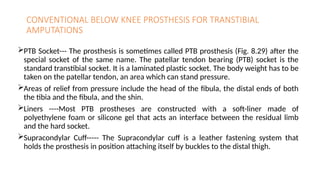
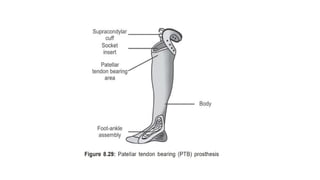
CONVENTIONAL BELOW KNEEPROSTHESIS FOR TRANSTIBIAL
AMPUTATIONS
PTB Socket--- The prosthesis is sometimes called PTB prosthesis (Fig. 8.29) after the
special socket of the same name. The patellar tendon bearing (PTB) socket is the
standard transtibial socket. It is a laminated plastic socket. The body weight has to be
taken on the patellar tendon, an area which can stand pressure.
Areas of relief from pressure include the head of the fibula, the distal ends of both
the tibia and the fibula, and the shin.
Liners ----Most PTB prostheses are constructed with a soft-liner made of
polyethylene foam or silicone gel that acts an interface between the residual limb
and the hard socket.
Supracondylar Cuff----- The Supracondylar cuff is a leather fastening system that
holds the prosthesis in position attaching itself by buckles to the distal thigh.
69.
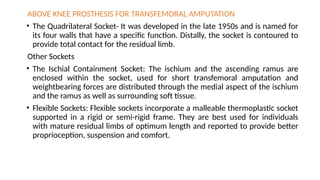
ABOVE KNEE PROSTHESISFOR TRANSFEMORAL AMPUTATION
• The Quadrilateral Socket- It was developed in the late 1950s and is named for
its four walls that have a specific function. Distally, the socket is contoured to
provide total contact for the residual limb.
Other Sockets
• The Ischial Containment Socket: The ischium and the ascending ramus are
enclosed within the socket, used for short transfemoral amputation and
weightbearing forces are distributed through the medial aspect of the ischium
and the ramus as well as surrounding soft tissue.
• Flexible Sockets: Flexible sockets incorporate a malleable thermoplastic socket
supported in a rigid or semi-rigid frame. They are best used for individuals
with mature residual limbs of optimum length and reported to provide better
proprioception, suspension and comfort.
70.
• Suspension Mechanisms
SilesianBand: The Silesian band is a soft strap of leather that is attached to the lateral
socket wall, encircles the pelvis, and connects with a strap on the anterior wall. The
Silesian band aids suspension and provides some control of rotation.
Pelvic Belt: The pelvic belt provides some mediolateral stability in patients whose
weight fluctuates widely.
72.
Prosthetic Training Phase
•Goals
• Continue to manage edema
• Continue with increasing UE and LE strength
• Continue with promoting mobility and self-care
• Incorporate use of prosthesis into all activities
• Maintain skin integrity
• Promote sound limb care
• Assist with limb loss adjustment
• EDUCATE, EDUCATE, EDUCATE!
73.
Factors That ContributeTo An Efficient Prosthetic Gait
• Accept the weight of the body on each leg.
• Balance on one foot in single-limb support.
• Advance each limb forward and prepare for the next step.
• Adapt to environmental demands.
82.
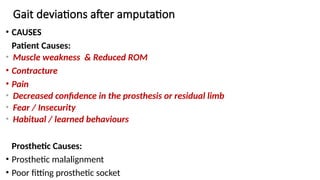
Gait deviations afteramputation
• CAUSES
Patient Causes:
• Muscle weakness & Reduced ROM
• Contracture
• Pain
• Decreased confidence in the prosthesis or residual limb
• Fear / Insecurity
• Habitual / learned behaviours
Prosthetic Causes:
• Prosthetic malalignment
• Poor fitting prosthetic socket
TRANSTIBIAL DESCRIPTION CAUSES
Absentknee flexion Knee fully extended at heel
strike
•Faulty suspension of the prosthesis – too
soft heel cushion or plantar flexor bumpers
•Foot placement too far forward on stepping
•Lack of pre-flexion of the socket
•Discomfort/pain
• Quads weakness
Excessive Knee
Flexion
Increased knee flexion at
heel strike (or mid stance),
patient feels as though
walking downhill
•Faulty suspension of prosthesis
•Prosthetic foot set in too much dorsiflexion
•Stiff heel cushion
•Flexion contracture of the knee
•Foot too posterior in relation to socket
85.
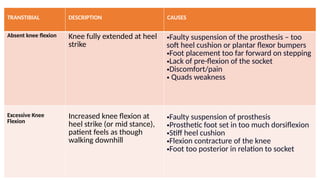
TRANSTIBIAL DESCRIPTION CAUSES
External
Rotationof
Foot at Heel
Strike
External rotation of the
prosthesis/foot at heel
strike.
•heel to hard
•Loose socket
Knee instability Knee flexion ‘jerky’ in
presentation during heel
strike to foot flat
Weak Quadriceps
Valgus/Varus
Moment
Knee shifts medially or
laterally during prosthetic
stance phase
•Foot placement (medial placement causes
lateral thrust and vice versa)
•Foot alignment on the prosthesis
•Socket loose
86.
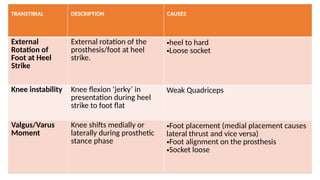
TRANSTIBIAL DESCRIPTION CAUSES
DropOff Heel off occurs too early
causing early knee flexion
•Foot too posterior on the prosthesis in
relation to the socket
•Excessive dorsiflexion of the foot on the
prosthesis
•Soft heel bumper on the prosthesis
Knee
Hyperextension
•Delayed heel causing
hyperextension of the
knee,
•walking up hill sensation
•Foot set too far forward on the prosthesis
in relation to socket
•Too hard a heel cushion
•Too much plantar flexion on the foot
Whip During swing phase foot
‘whips’ laterally or
medially
•Poor suspension
•Knee internally or externally rotated
87.
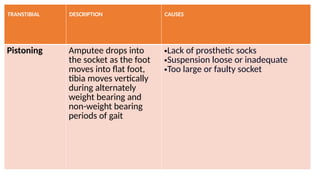
TRANSTIBIAL DESCRIPTION CAUSES
PistoningAmputee drops into
the socket as the foot
moves into flat foot,
tibia moves vertically
during alternately
weight bearing and
non-weight bearing
periods of gait
•Lack of prosthetic socks
•Suspension loose or inadequate
•Too large or faulty socket
TRANSFEMO-RAL DESCRIPTION CAUSES
ProstheticInstability The prosthetic knee has a tendency
to buckle on weight bearing
•Knee set too far anterior
•Heel cushion too firm
•Weak hip extensors
•Heel of the shoe too high causing the pylon of the
prosthesis to move anteriorly
•Severe hip flexion contracture
Foot Slap Foot progresses too quickly from
heel strike to foot flat, creating a
slapping noise
•Patient forcing foot contact to gain knee stability
•Heel cushion too soft
•Plantar flexion cushion too soft Excessive dorsiflexion
90.
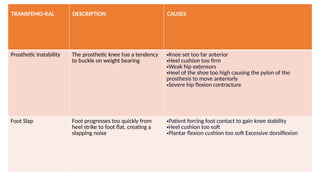
TRANSFEMORAL DESCRIPTION CAUSES
AbductedGait Increased base of support during
mobility, prosthetic foot placement
is lateral to the normal foot
placement during the gait cycle
•Prosthesis too long
•Socket too small
•Suspension belt may be insufficient-band may be too far
from the ileum
•Pain in the groin or medial wall of the prosthesis
•Hip abductor contractures
•Lateral wall of the prosthesis not supporting the femur
sufficiently
•Socket of prosthesis abducted in alignment
•Fear/lack of confidence transferring weight onto
prosthesis
•Alignment of the lower half of the pylon of the prosthesis
in relation to socket
91.
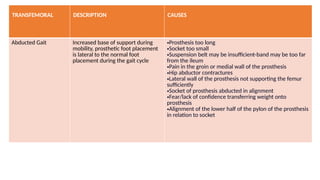
TRANSFEMORAL DESCRIPTION •CAUSES
LateralTrunk Bending Trunk flexes towards prosthesis
during prosthetic stance phase
•Prosthesis too short
•Short stump length
•Weak or contracted hip abductors
•Foot outset excessively in relation to socket
•Lack of prosthetic lateral wall support
•Pain on the lateral distal end of the stump
•Lack of balance
•Habit
Anterior Trunk
Bending
Trunk flexes forwards during
prosthetic stance phase
92.
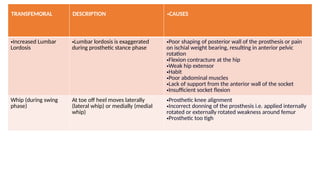
TRANSFEMORAL DESCRIPTION •CAUSES
•IncreasedLumbar
Lordosis
•Lumbar lordosis is exaggerated
during prosthetic stance phase
•Poor shaping of posterior wall of the prosthesis or pain
on ischial weight bearing, resulting in anterior pelvic
rotation
•Flexion contracture at the hip
•Weak hip extensor
•Habit
•Poor abdominal muscles
•Lack of support from the anterior wall of the socket
•Insufficient socket flexion
Whip (during swing
phase)
At toe off heel moves laterally
(lateral whip) or medially (medial
whip)
•Prosthetic knee alignment
•Incorrect donning of the prosthesis i.e. applied internally
rotated or externally rotated weakness around femur
•Prosthetic too tigh
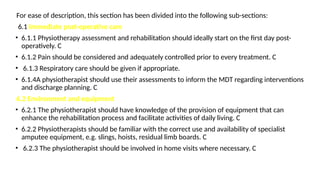
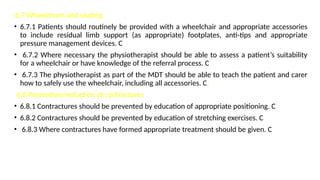
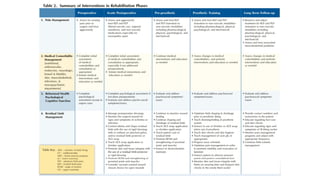
93.
TRANSFEMORAL DESCRIPTION •CAUSES
PistoningSocket dropping off when prosthesis
lifted
•Insufficient suspension
•Socket too loose[2]
or delayed knee flexion during toe off
(‘free knee only’) caused by increased resistance of the
prosthesis
•Alignment of prosthesis
Excessive Heel Rise Prosthetic heel rises more than
sound side
•Lack of friction on prosthetic knee
•Amputee generating more force then required to gain
knee flexion
•Poor/lack of extension aid
Reduced Heel Rise Prosthetic heel does not rise as
much as sound side
•Locked knee
•Lack of hip flexion
•Too much friction on free knee
•Extension aid to tight
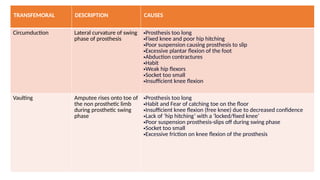
94.
TRANSFEMORAL DESCRIPTION CAUSES
CircumductionLateral curvature of swing
phase of prosthesis
•Prosthesis too long
•Fixed knee and poor hip hitching
•Poor suspension causing prosthesis to slip
•Excessive plantar flexion of the foot
•Abduction contractures
•Habit
•Weak hip flexors
•Socket too small
•Insufficient knee flexion
Vaulting Amputee rises onto toe of
the non prosthetic limb
during prosthetic swing
phase
•Prosthesis too long
•Habit and Fear of catching toe on the floor
•Insufficient knee flexion (free knee) due to decreased confidence
•Lack of ‘hip hitching’ with a ‘locked/fixed knee’
•Poor suspension prosthesis-slips off during swing phase
•Socket too small
•Excessive friction on knee flexion of the prosthesis
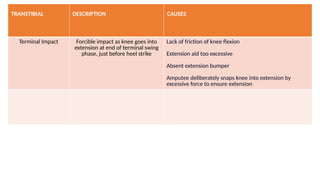
95.
TRANSTIBIAL DESCRIPTION CAUSES
TerminalImpact Forcible impact as knee goes into
extension at end of terminal swing
phase, just before heel strike
Lack of friction of knee flexion
Extension aid too excessive
Absent extension bumper
Amputee deliberately snaps knee into extension by
excessive force to ensure extension
96.
Exercises to improvedeviations
• Lateral weight shifting – parallel bars
• Forward and back weight shifting – pelvic movement
• High stepping – with amputee leg
• Balance board
• Throwing and catching
• Obstacle stepping
• Football
• Braiding -swings one leg across the front of the body and then behind
• Single leg standing
• Gait Re-Education
• ( all should be done in parallel bar with both hand supported and progression should be with one
hand support or no support. And then on floor)
97.
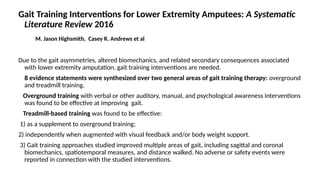
Gait Training Interventionsfor Lower Extremity Amputees: A Systematic
Literature Review 2016
M. Jason Highsmith, Casey R. Andrews et al
Due to the gait asymmetries, altered biomechanics, and related secondary consequences associated
with lower extremity amputation, gait training interventions are needed.
8 evidence statements were synthesized over two general areas of gait training therapy: overground
and treadmill training.
Overground training with verbal or other auditory, manual, and psychological awareness interventions
was found to be effective at improving gait.
Treadmill-based training was found to be effective:
1) as a supplement to overground training;
2) independently when augmented with visual feedback and/or body weight support.
3) Gait training approaches studied improved multiple areas of gait, including sagittal and coronal
biomechanics, spatiotemporal measures, and distance walked. No adverse or safety events were
reported in connection with the studied interventions.
98.
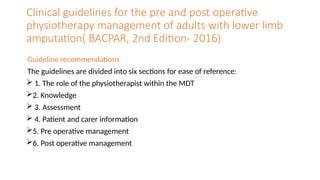
Clinical guidelines forthe pre and post operative
physiotherapy management of adults with lower limb
amputation( BACPAR, 2nd Edition- 2016)
Guideline recommendations
The guidelines are divided into six sections for ease of reference:
1. The role of the physiotherapist within the MDT
2. Knowledge
3. Assessment
4. Patient and carer information
5. Pre operative management
6. Post operative management
99.
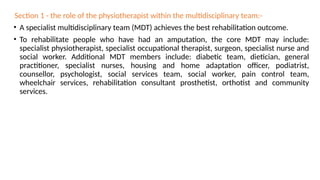
Section 1 -the role of the physiotherapist within the multidisciplinary team:-
• A specialist multidisciplinary team (MDT) achieves the best rehabilitation outcome.
• To rehabilitate people who have had an amputation, the core MDT may include:
specialist physiotherapist, specialist occupational therapist, surgeon, specialist nurse and
social worker. Additional MDT members include: diabetic team, dietician, general
practitioner, specialist nurses, housing and home adaptation officer, podiatrist,
counsellor, psychologist, social services team, social worker, pain control team,
wheelchair services, rehabilitation consultant prosthetist, orthotist and community
services.
100.
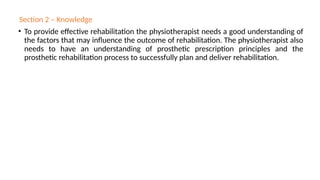
Section 2 –Knowledge
• To provide effective rehabilitation the physiotherapist needs a good understanding of
the factors that may influence the outcome of rehabilitation. The physiotherapist also
needs to have an understanding of prosthetic prescription principles and the
prosthetic rehabilitation process to successfully plan and deliver rehabilitation.
101.
Section 3 –Assessment
• This should take into account the emotional and cognitive status and co-morbidities
e.g. cardiac and/or renal disease, diabetes, arthritis or previous stroke, which may
affect the patient’s motivation, exercise tolerance, skin condition or sensation. The
social situation, including available support, occupation and hobbies, together with the
home environment of the patient, should also be considered.
102.
Section 4 –Patient and Carer Information
The CSP Quality Assurance Standard states that “information [should be]
provided to enable service users to participate fully in their care”. This promotes
understanding of the process and reasoning behind treatment. The
rehabilitation process should have an educational element that empowers
patients and carers to take an active role in their present and future
management. This will assist with problem solving and awareness of when to
seek professional help. Due to the number of recommendations in this section it
has been sub-divided into four sections for ease of use. These subsections are:
4.1 Patient journey
4.2 Informed goal setting
4.3 Care of the remaining limb
4.4 Care of the residual limb
103.
Section 5 –Pre-op Management
Early assessment and planning of rehabilitation can commence at this stage and helps to
prepare the patient for rehabilitation. A pre-amputation consultation also enables the
physiotherapist to give appropriate advice, information and reassurance; issues such as
phantom limb sensation and avoidance of falls may be discussed. However, it is
acknowledged that patients who require emergency amputation may not have the
opportunity for pre-amputation consultation, assessment and treatment.
Recommendations
5.1 Where possible the physiotherapist should reinforce information given by other
MDT members about the general surgical process (not technique). C
5.2 Where possible the patient and carers should be given advice, information and
reassurance by the physiotherapist about rehabilitation. C
5.3 The physiotherapy assessment should be commenced preoperatively, if possible. C
104.
• 5.4 Wherepossible rehabilitation/discharge planning should commence pre-operatively.
• 5.5 Where appropriate and possible the patient should be instructed in wheelchair use pre-
operatively. C
• 5.6 A structured exercise regime should be started as early as possible. C
• 5.7 Bed mobility should be taught where possible. C
• 5.8 Where appropriate and possible transfers should be taught pre-operatively. C
• 5.9 If indicated, the patient should be assessed for physiotherapy respiratory care. C
• 5.10 If indicated, the patient should be given appropriate physiotherapy respiratory
treatment. C
• 5.11 Pain control should be optimised prior to physiotherapy treatment pre-operatively. C
• 5.12 If appropriate, and with the patient’s consent, carers should be involved in pre-operative
treatment and exercise programmes. C
105.
• Section 6– Post-op Management
• The rehabilitation process should commence as early as possible, preferably following
a suitable care pathway. Patients should be assessed and a rehabilitation plan discussed
and agreed. Advice and information should be given regarding bed mobility, to avoid
complications such as contractures and pressure sores. Appropriate advice and
assistance with transfers should be given. Following assessment, a problem list should
be made, with both short and long term goals considered, taking into account the
patient’s psychological, emotional and physical status, pain management and the
broader issues surrounding social and home environment.
106.
For ease ofdescription, this section has been divided into the following sub-sections:
6.1 Immediate post-operative care
• 6.1.1 Physiotherapy assessment and rehabilitation should ideally start on the first day post-
operatively. C
• 6.1.2 Pain should be considered and adequately controlled prior to every treatment. C
• 6.1.3 Respiratory care should be given if appropriate.
• 6.1.4A physiotherapist should use their assessments to inform the MDT regarding interventions
and discharge planning. C
6.2 Environment and equipment
• 6.2.1 The physiotherapist should have knowledge of the provision of equipment that can
enhance the rehabilitation process and facilitate activities of daily living. C
• 6.2.2 Physiotherapists should be familiar with the correct use and availability of specialist
amputee equipment, e.g. slings, hoists, residual limb boards. C
• 6.2.3 The physiotherapist should be involved in home visits where necessary. C
107.
6.3 Compression therapy
•6.3.1 A compression sock should be used in preference to elastic bandages for reducing
limb volume. D
• 6.3.2 The physiotherapist should use compression therapy as appropriate. D
• 6.3.3 The timing of compression therapy application should be discussed with the MDT
at an early stage. C
108.
6.4 Mobility
• 6.4.1Ideally, bed mobility should be taught on the first day post-operatively. C
• 6.4.2 Sitting balance should be re-educated if needed. C
• 6.4.3 Standing balance should be re-educated if needed. C
• 6.4.4 Safe transfers should be taught as early as possible. C
• 6.4.5 Mobility post-operatively should be in a wheelchair unless there are specified
reasons to teach a patient to use crutches/zimmer frame/rollator. C
• 6.4.6 The physiotherapist should help the patient gain maximum mobility post-
operatively. C
109.
6.5 Early walkingaids (EWAs
• 6.5.1 EWAs should be considered as part of the rehabilitation programme for all lower limb
amputation patients as an assessment tool. B
• 6.5.2 EWAs should be considered as part of the rehabilitation programme for all lower limb
amputation patients as a treatment tool. B
• 6.5.3 EWAs should be used under the supervision of therapists trained in their correct and
safe application and use. C
• 6.6 Falls management
• 6.6.1 The patient, carers and the MDT should be made aware that the risk of falling is
increased following lower limb amputation. B
• 6.6.2 Rehabilitation programmes should include education on preventing falls. B
• 6.6.3 Patients and carers should be given instructions on how to get up from the floor in the
event of the patient falling. B
• 6.6.4 Advice should be given in the event that the patient is unable to rise from the floor. B
110.
6.7 Wheelchairs andseating
• 6.7.1 Patients should routinely be provided with a wheelchair and appropriate accessories
to include residual limb support (as appropriate) footplates, anti-tips and appropriate
pressure management devices. C
• 6.7.2 Where necessary the physiotherapist should be able to assess a patient’s suitability
for a wheelchair or have knowledge of the referral process. C
• 6.7.3 The physiotherapist as part of the MDT should be able to teach the patient and carer
how to safely use the wheelchair, including all accessories. C.
6.8 Prevention/reduction of contractures
• 6.8.1 Contractures should be prevented by education of appropriate positioning. C
• 6.8.2 Contractures should be prevented by education of stretching exercises. C
• 6.8.3 Where contractures have formed appropriate treatment should be given. C
111.
6.9 Exercise programmes
•6.9.1 Following on from the initial assessment, an exercise program should be provided to
address the problems identified. This should be reviewed and progressed as appropriate. C
• 6.9.2 An exercise regime should be given relevant to the patient’s goals and reviewed on a
regular basis. C
• 6.10 Management of phantom sensation and pain
• 6.10.1 As early as possible, patients should be made aware they may experience phantom
limb sensation or pain postoperatively. B6.10.2 Information and treatment regarding
phantom limb sensation and pain should be given by clinicians with appropriate
knowledge and training. B
• 6.10.3 Techniques for the self-management of phantom sensation and/or pain should be
taught. C
• 6.10.4 Appropriate information and treatment should be given for residual limb pain. C
REFRENCES
• Amputation andprosthetic ; Bella j. May 2nd
edition
• Physical rehabilitation . Susan B O’sullivan. 5th edition, 2006.
• S Sunder , textbook of rehabilitation , 3rd
edition.
• va/dod clinical practice guideline for rehabilitation of lower limb
amputation a m p u tat i o n department of veterans affairs department
of defense guideline summary , January 2008
• BACPAR, 2016








![TRANSFEMORAL DESCRIPTION •CAUSES
Pistoning Socket dropping off when prosthesis
lifted
•Insufficient suspension
•Socket too loose[2]
or delayed knee flexion during toe off
(‘free knee only’) caused by increased resistance of the
prosthesis
•Alignment of prosthesis
Excessive Heel Rise Prosthetic heel rises more than
sound side
•Lack of friction on prosthetic knee
•Amputee generating more force then required to gain
knee flexion
•Poor/lack of extension aid
Reduced Heel Rise Prosthetic heel does not rise as
much as sound side
•Locked knee
•Lack of hip flexion
•Too much friction on free knee
•Extension aid to tight](https://image.slidesharecdn.com/lowerlimbamputationseminar-250331121821-4d0372f2/85/LOWER-LIMB-AMPUTATION-Amputation-is-the-surgical-removal-of-a-limb-or-part-of-a-limb-often-necessary-due-to-severe-injury-infection-or-disease-such-as-cancer-or-peripheral-vascular-disease-93-320.jpg)
![Section 4 – Patient and Carer Information
The CSP Quality Assurance Standard states that “information [should be]
provided to enable service users to participate fully in their care”. This promotes
understanding of the process and reasoning behind treatment. The
rehabilitation process should have an educational element that empowers
patients and carers to take an active role in their present and future
management. This will assist with problem solving and awareness of when to
seek professional help. Due to the number of recommendations in this section it
has been sub-divided into four sections for ease of use. These subsections are:
4.1 Patient journey
4.2 Informed goal setting
4.3 Care of the remaining limb
4.4 Care of the residual limb](https://image.slidesharecdn.com/lowerlimbamputationseminar-250331121821-4d0372f2/85/LOWER-LIMB-AMPUTATION-Amputation-is-the-surgical-removal-of-a-limb-or-part-of-a-limb-often-necessary-due-to-severe-injury-infection-or-disease-such-as-cancer-or-peripheral-vascular-disease-102-320.jpg)





![LOWER LIMB AMPUTATION SO much for [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lowerlimbamputations1-240930130033-23e44db1-thumbnail.jpg?width=640&height=640&fit=bounds)










































