Presentation1, radiological imaging of gastro intestinal stromal tumour(gist).
•Download as PPTX, PDF•
21 likes•3,612 views

This document summarizes radiological imaging of gastrointestinal stromal tumors (GISTs). It describes GISTs as the most common mesenchymal tumors of the GI tract, occurring most often in older adults. Imaging findings are discussed for various modalities including CT, MRI, US, and PET. Characteristic features include soft tissue masses arising from the GI tract wall. Larger tumors may show necrosis, hemorrhage, or cystic changes. Imaging can also detect metastatic lesions or tumor response to chemotherapy.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1, radiological imaging of gastro intestinal stromal tumour(gist).
Similar to Presentation1, radiological imaging of gastro intestinal stromal tumour(gist). (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of gastro intestinal stromal tumour(gist).
- 1. Radiological Imaging of Gastrointestinal stromal tumor. Dr/ ABD ALLAH NAZEER. MD.
- 2. Gastrointestinal stromal tumours (GIST) are the most common mesenchymal tumours of the gastrointestinal tract. They account for ~5% of all sarcomas. They respond remarkably well to chemotherapy. Terminology Previously these tumours have been variably referred to as leiomyomas, leiomyosarcomas, leiomyoblastomas. Epidemiology GISTs usually occurs after the age of 40, with most seen in older patients except when associated with tumour syndromes when they may present earlier and are often multiple. It is equal in both male and female with possible slight male predilection. Clinical presentation Clinical presentation is variable and reflects the variability of radiographic appearances, location and biological behavior. Many tumours are incidentally identified on imaging for other indications but mostly present with dysphagia. Some tumours, on the other hand, are aggressive and present with metastases or symptoms relating to local disease. Ulceration is seen in 50% of tumours although it is commoner in large tumours. Hemorrhage may occur, with presentation relating to gastrointestinal bleeding.
- 3. Pathology GISTs are believed to arise from the interstitial cells of Cajal, with 95% staining positive for CD117 (c-KIT) and 70% for CD34. The former is a tyrosine kinase growth factor receptor and the target of ST-571 (imatinib/Gleevec/GlivecTM) . As the tumours are intramural but submucosal, the overlying mucosa often appears intact on pathological and imaging assessment. Grading GISTs requires assessment of both tumour size and mitotic index. Smaller lesions have less aggressive biological behavior, as do stomach GISTs when compared to tumours elsewhere along the gastrointestinal tract. Macroscopic appearance They are rounded with frequent hemorrhage. Larger tumours may also demonstrate necrosis and cystic change. Size is variable, ranging from 1 to 30 cm. Histology Histology demonstrates a relatively cellular tumour composed of spindle cells (70- 80%) and plump epithelioid cells (20-30%). They appear to arise from the muscularis propria layer. Associations The vast majority of GISTs are sporadic. However, they occasionally occur in the setting of a recognized syndrome, including: Carney triad neurofibromatosis type 1 (NF1).
- 4. Location and classification Common sites of involvement include stomach: 70% small intestine: 20-25% anorectum: 7% colon esophagus GISTs occur not only anywhere along the gastrointestinal tract, but also in the mesentery, omentum and retroperitoneum, these are then called extra-gastrointestinal GISTs. Metastatic lesions may also be seen in cases of malignant extra- gastrointestinal GISTs. Radiographic features Specific appearances will vary according to location, but in general, these tumours appear as rounded soft tissue masses, arising from the wall of a hollow viscus (most commonly the stomach) and projecting into the lumen, or less commonly outwards from the serosa. Mucosal ulceration is present in 50% of cases with large necrotic cavities communicating with the lumen also seen.
- 5. Plain radiograph When large, soft tissue density displacing bowel loops may be seen, which is, of course, non-specific. Fluoroscopy On upper abdominal studies, filling defect projecting from the wall of the stomach may be seen, with overlying ulceration or cavitation. The tumour margins are normally seen as smooth and may form right or obtuse angles with the adjacent mucosa due to its intramural origin. CT Appearances vary with size and location. Typically the mass is of soft tissue density with central areas of lower density when necrosis is present (usually in larger tumours) that occasionally appear as fluid-fluid levels. As the tumours are often exophytic, it can be difficult to delineate them on CT if the stomach is distended with barium, though the non-enhancing central necrotic area may be helpful. A deep crescent-shaped ulceration demonstrating an internal air-fluid level may be referred to as the Torricelli-Bernoulli sign. Enhancement is typically peripheral (due to central necrosis). Calcification is uncommon (3%). Metastases (distant, peritoneal, omental) or direct invasion into adjacent organs may be seen in more aggressive lesions. Lymph node enlargement is not a feature
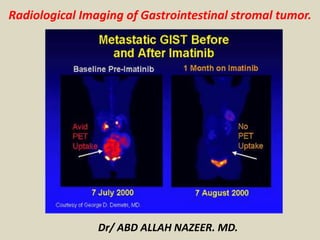
- 6. US: Typically hypoechoic, Variable vascularity on color Doppler and usually difficult to identify organ of origin. MRI Presence of necrosis, hemorrhagic and cystic change make appearances variable: T1: low signal intensity solid component enhancement is usually present, and predominantly peripheral in larger lesions T2: high signal intensity solid component. T1 post-contrast: Enhancement of solid areas and non-enhancing regions consistent with necrosis or hemorrhage. Angiography: SMA angiogram show hypervascular GIST and the tumour blush on arteriogram. 18 FDG-PET, PET/CT: Metabolic responses to imatinib treatment can be followed using positron emission tomography(PET) using fluorine-18-flourodeoxyglucose(18 FDG). Significant reduction in tumour 18FDG uptake in imatinib –responsive tumors as early as 24 hours later and by 1 month after initiating imatinib therapy. Lack of metabolic response on 18FD-PET indicates primary or secondary resistance to chromo therapeutic agent.
- 7. Ilial perivesical GIST, appearing on ultrasound as an hypoechoic mass, markedly heterogeneous and slightly lobulated.
- 8. Endoscopic Ultrasonography (EU) of a duodenal bulb GIST, with calcifications on its deeper segment.
- 9. EU of a large gastric body GIST, with areas of necrosis and hemorrhage.
- 10. Cystic GIST. Longitudinal USG scan of the abdomen (A) in a 41-year-old male shows a predominantly cystic mass with septae (arrows) in the left hypochondrium. Axial contrast-enhanced CT scan (B) shows a peripherally enhancing cystic mass (arrow) in the lesser sac region along the tail of the pancreas.
- 11. Gastric gastrointestinal stromal tumor (GIST) en face. Upper GI image obtained during the single contrast enhancement portion shows an incidentally found mass. The smooth borders suggest a submucosal process. At surgery, a GIST was found.
- 12. Multifocal gastrointestinal stromal tumors. Barium examination and CT Scan reveals a smooth mass that causes narrowing in the second portion of the duodenum (arrows).
- 13. Malignant GIST. Barium meal study (A) shows an irregular filling defect along the fundus and greater curvature of the stomach, suggestive of ulceration (arrow). Axial contrast-enhanced CT scan (B) shows an exophytic heterogeneously enhancing mass (arrowhead) arising from the stomach (small arrow) with areas of ulceration (long arrow)
- 14. Small-bowel gastrointestinal stromal tumor with a diffusely thickened bowel wall.
- 15. Gastric gastrointestinal stromal tumor (GIST) en face. Upper GI image obtained during the single contrast enhancement portion shows an incidentally found mass. The smooth borders suggest a submucosal process. At surgery, a GIST was found.
- 16. Gastric gastrointestinal stromal tumor with huge exophytic component, which has become ulcerated. Barium collects in the exophytic ulcer crater (arrows). CT demonstrates the GIST with large exophytic ulceration (arrows).
- 17. Proximal jejunal gastrointestinal stromal tumor that is completely exophytic and not visible at small- bowel barium examination. Contrast-enhanced CT obtained in the same patient as in the previous image demonstrates a peripherally enhancing mass immediately adjacent to the pancreas that was thought to be a pancreatic neoplasm. However, at surgery, this proved to be a proximal exophytic jejunal GIST.
- 18. Gastrointestinal stromal tumor. Enteroclysis results were surprisingly normal. No abnormalities are seen, and no significant mass effect suggests the presence of the mass. Gastrointestinal stromal tumor (GIST). CT demonstrates a complex mass originating from the small bowel with characteristics of a GIST.
- 32. Massive ileal GIST, with invasion of adjacent bowel loops. Note the small calcification at the bottom portion of the mass.
- 33. Large gastric GIST on a T2-weighted MRI, with areas of hemorrhage and necrosis.
- 34. T2-weighted MRI: large rectal GIST with mild hyperintensity relative to skeletal muscle.
- 35. Gastrointestinal stromal tumor (GIST). Patient in the previous image then underwent angiography, which demonstrates a mass (white arrows) in the same location as the small-bowel bleed. The blood supply is from the superior mesenteric artery (red arrow). Minimal mass effect on the bladder is noted (yellow arrows). Findings are consistent with a small bowel mass, which stained positive for CD117; this result is consistent with a GIST.
- 36. GIST of the jejunum in a 53-year-old woman with acute GI bleeding. CT show prominent feeding and draining veins (c) Digital subtraction angiography shows a hypervascular mass (arrows) fed by branches of the superior mesenteric artery (arrowhead).
- 37. Larger and multiple small bowel gastrointestinal stromal tumors. A 52-year-old woman with 2 gastrointestinal stromal tumors in the middle jejunum. The tumors (white arrows) were 5.5 cm and 1.5 cm in diameter, respectively, and were also hypervascular and homogeneous in the early arterial phrase. The feeding artery of the large tumor (A: white arrowhead) was slightly thickened. The draining veins of the tumors (B: black arrowheads) were also clear. The pathological risk classification was high (large) and very low (small).
- 38. Small bowel gastrointestinal stromal tumor. A 70-year-old man with a 1.2 cm gastrointestinal stromal tumor of very low risk classification in the upper jejunum. The tumor (white arrows) was round, well-defined and homogeneous in the early arterial phase (A, B). The feeding arteries were not significantly enlarged, and the draining veins (B: black arrowheads) developed clearly and early, merging into the portal vein system (B, asterisk).
- 39. Small bowel gastrointestinal stromal tumor case with active bleeding. A 35-year-old woman with a 3.2 cm gastrointestinal stromal tumor in the middle jejunum. The hemoglobin was 34 g/L. Digital subtraction angiography showed many draining veins (arrows) on the tumor merging into the portal vein system (arrowheads) without signs of active bleeding. The tumor was slightly lobular and was low risk based on the pathological classification.
- 40. Gastrointestinal stromal tumor. A 62-year-old women presented with 2 episodes of massive GI bleeding. Nuclear medicine GI bleed scanning demonstrates increased tracer activity in the mid abdomen (arrows) consistent with a small bowel active bleed.
- 42. This correlates with computed tomography (CT) scans, on this side shrinking. On this side, you see the PET scan is very hot, there is lots of uptake, then it goes cold. The speed of this is what has been amazing to all of us.
- 46. A 52-year-old man with suspected recurrence of gastrointestinal stromal tumors (GISTs). (A) An upper abdominal image reveals a 10- x 7-cm mass in the right liver lobe (arrow). (B) Mid abdominal image shows a 12- x 6-cm subhepatic mass (arrow). (C) A necrotic pelvic lymph node (arrow) measuring 3 x 3 cm was also noted. (D) A positron emission tomography scan with 18F-fluorodeoxyglucose (FDG) shows markedly increased uptake in the liver (short arrow) and the subhepatic masses (long arrow). Lack of FDG uptake in the pelvis excludes this mass as a GIST. Positron emission tomography helped in accurate restaging by revealing the malignant nature of the hepatic and subhepatic masses and excluding spread to the pelvis.
- 47. A 42-year-old woman with a history of surgical removal of gastrointestinal stromal tumor had a PET scan with 18F-fluorodeoxyglucose for restaging. (A) The positron emission tomography (PET) scan showed a small focus of markedly increased FDG uptake in the right lower neck (black arrow). (B) An ultrasound image revealed a hypoechoic lesion (white arrow) in the right lobe of the thyroid gland correlating with the abnormal uptake noted on the PET scan. Biopsy revealed an unsuspected incidental papillary carcinoma.
- 48. 41-year-old woman following partial resection of gastrointestinal stromal tumors. (A) Before therapy with Gleevec (Novartis Pharmaceuticals Corp., East Hanover, NJ), positron emission tomography (PET) shows markedly increased uptake in the left abdomen and 3 liver lesions (arrows). (B) A PET scan performed 5 weeks after the initiation of therapy was normal, with no abnormal uptake in the abdomen or liver, indicating an excellent tumor response to therapy. The uptake of 18F-fluorodeoxyglucose in the heart, renal collecting systems, and bladder is physiologic.
- 50. Thank You.