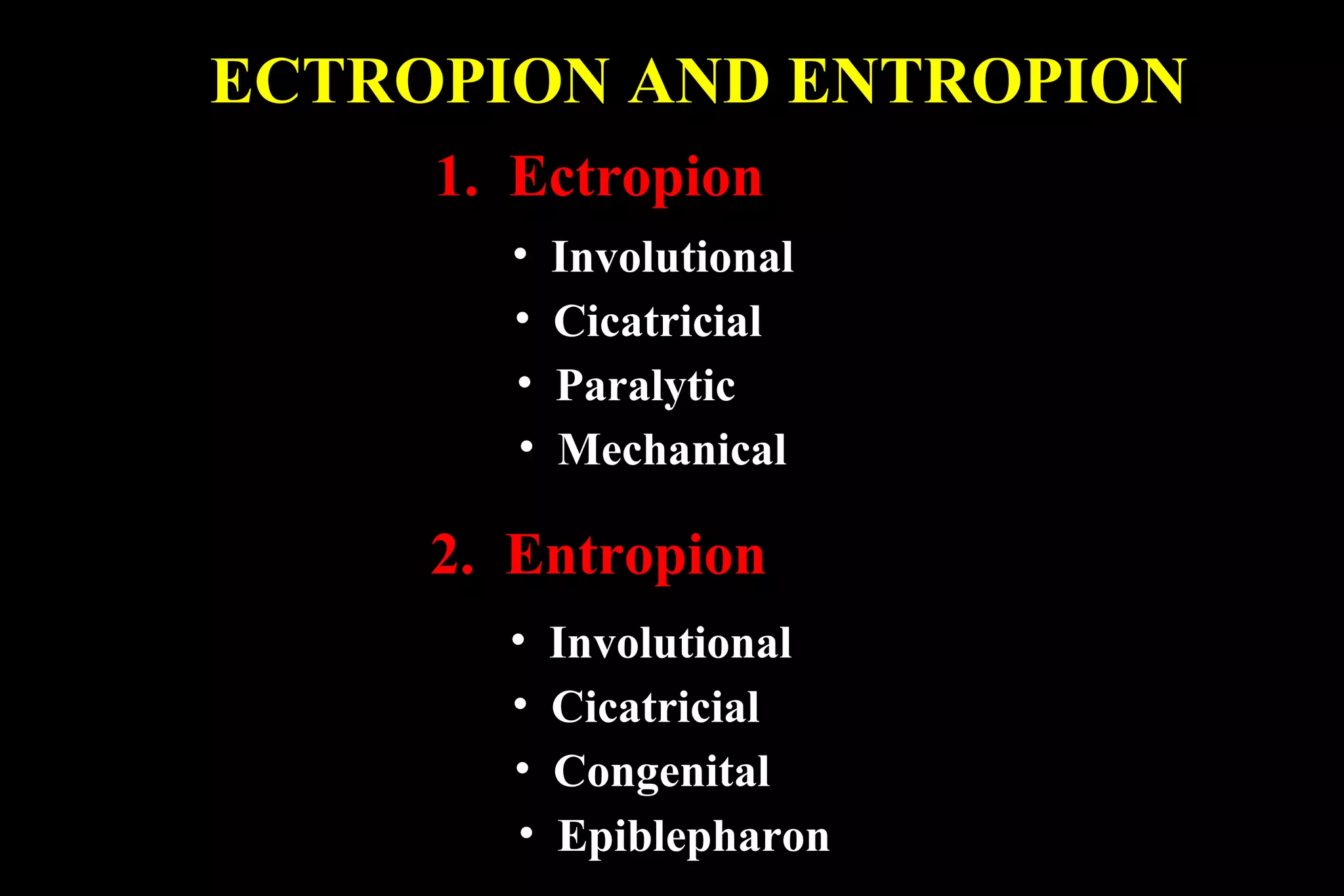
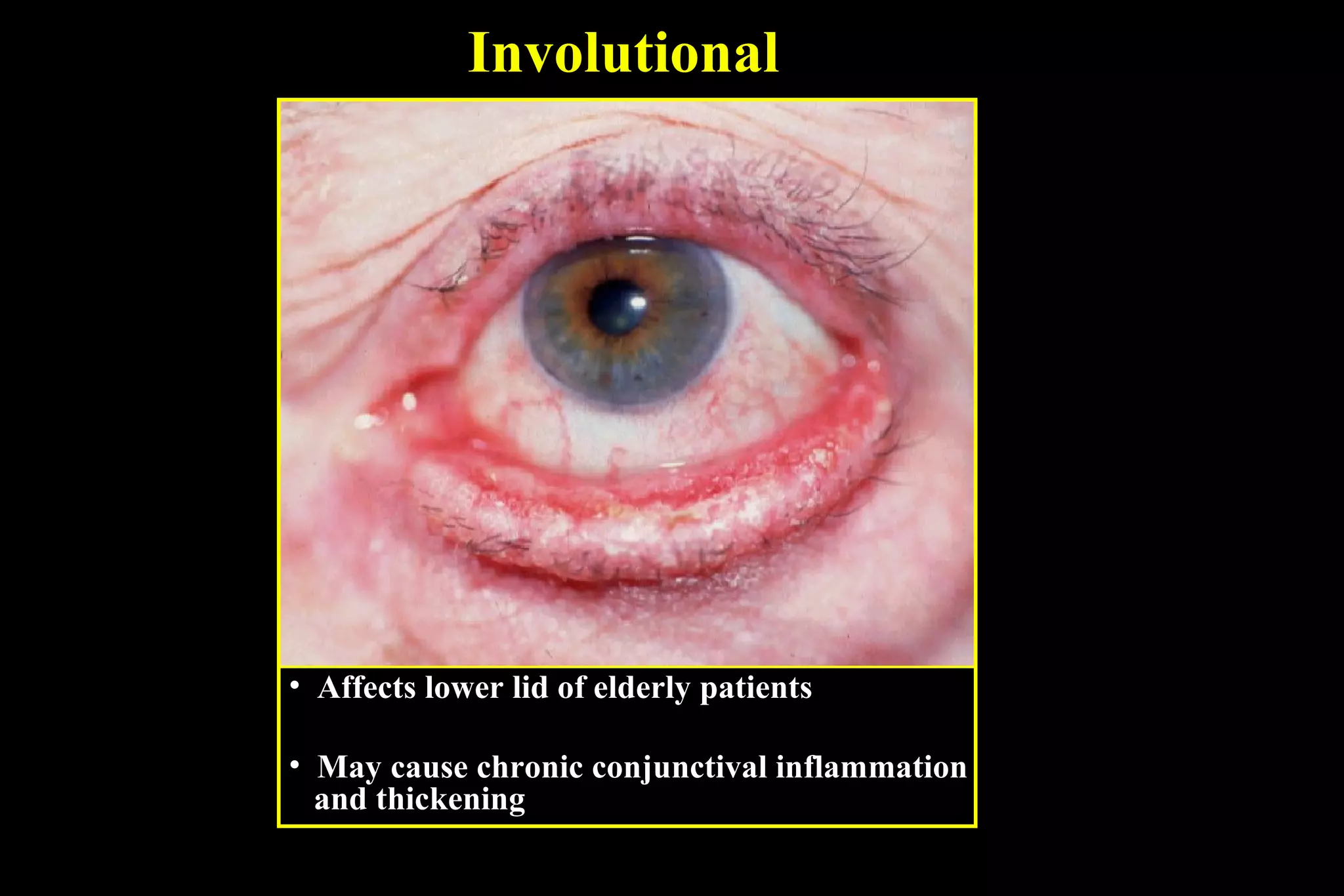
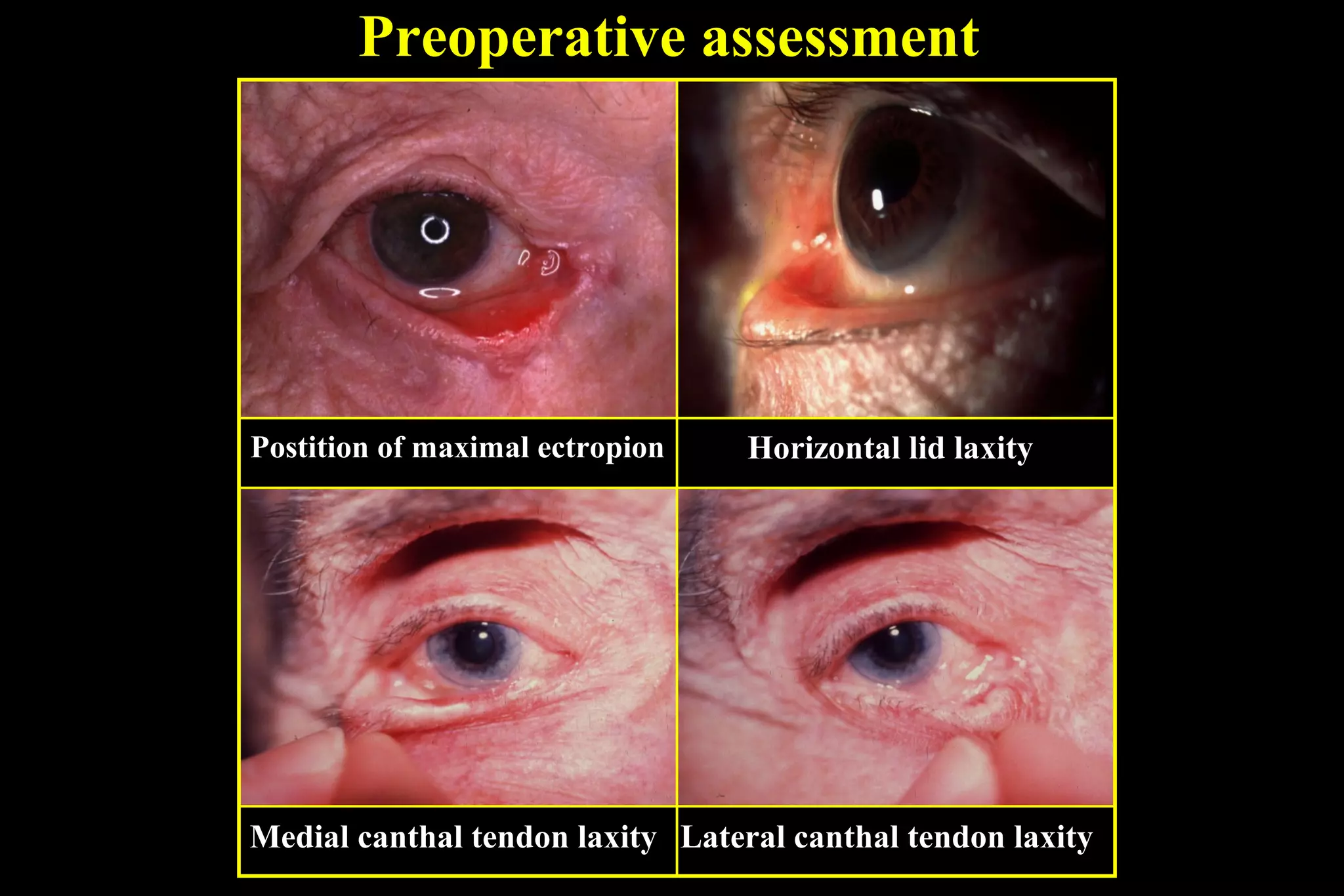
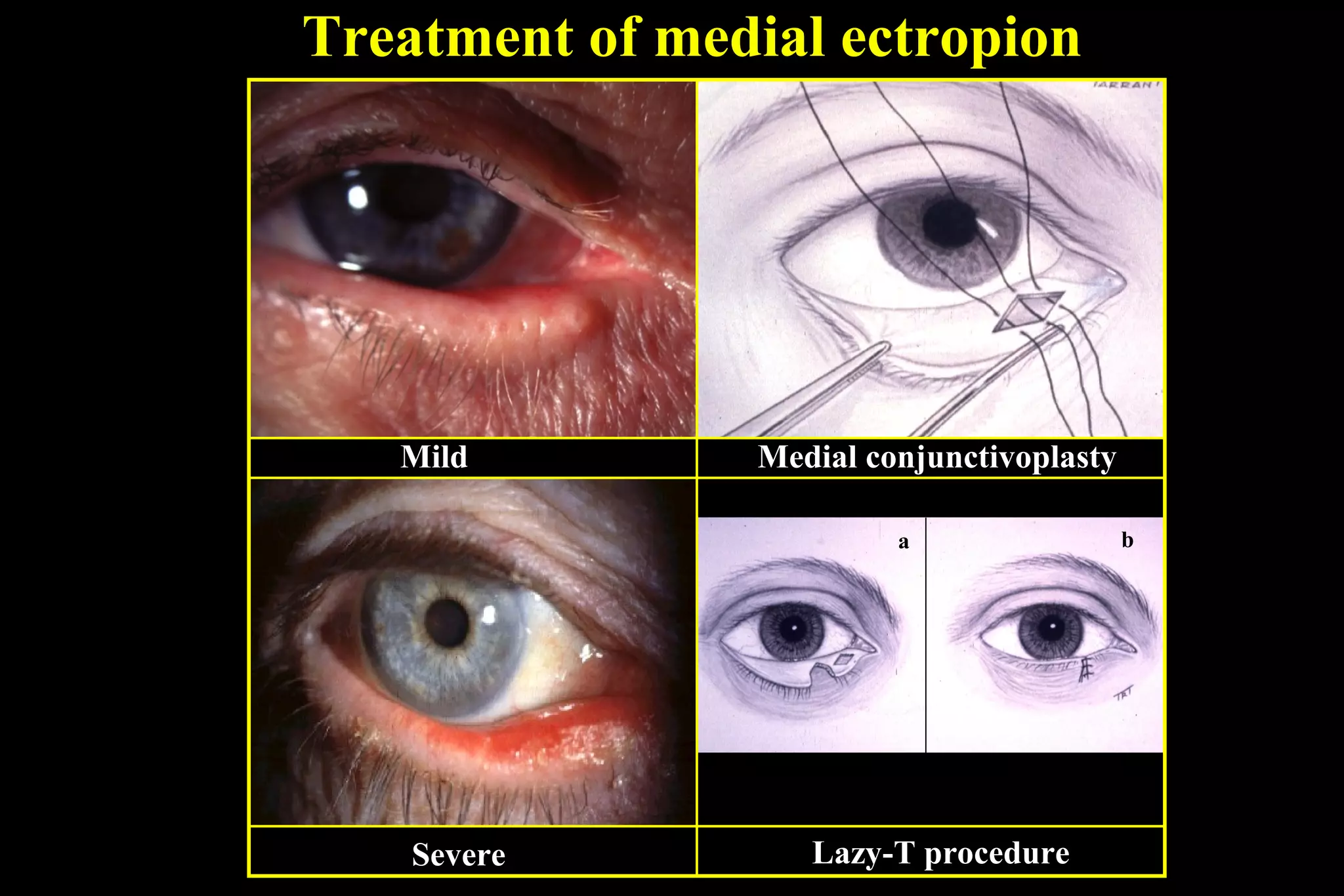
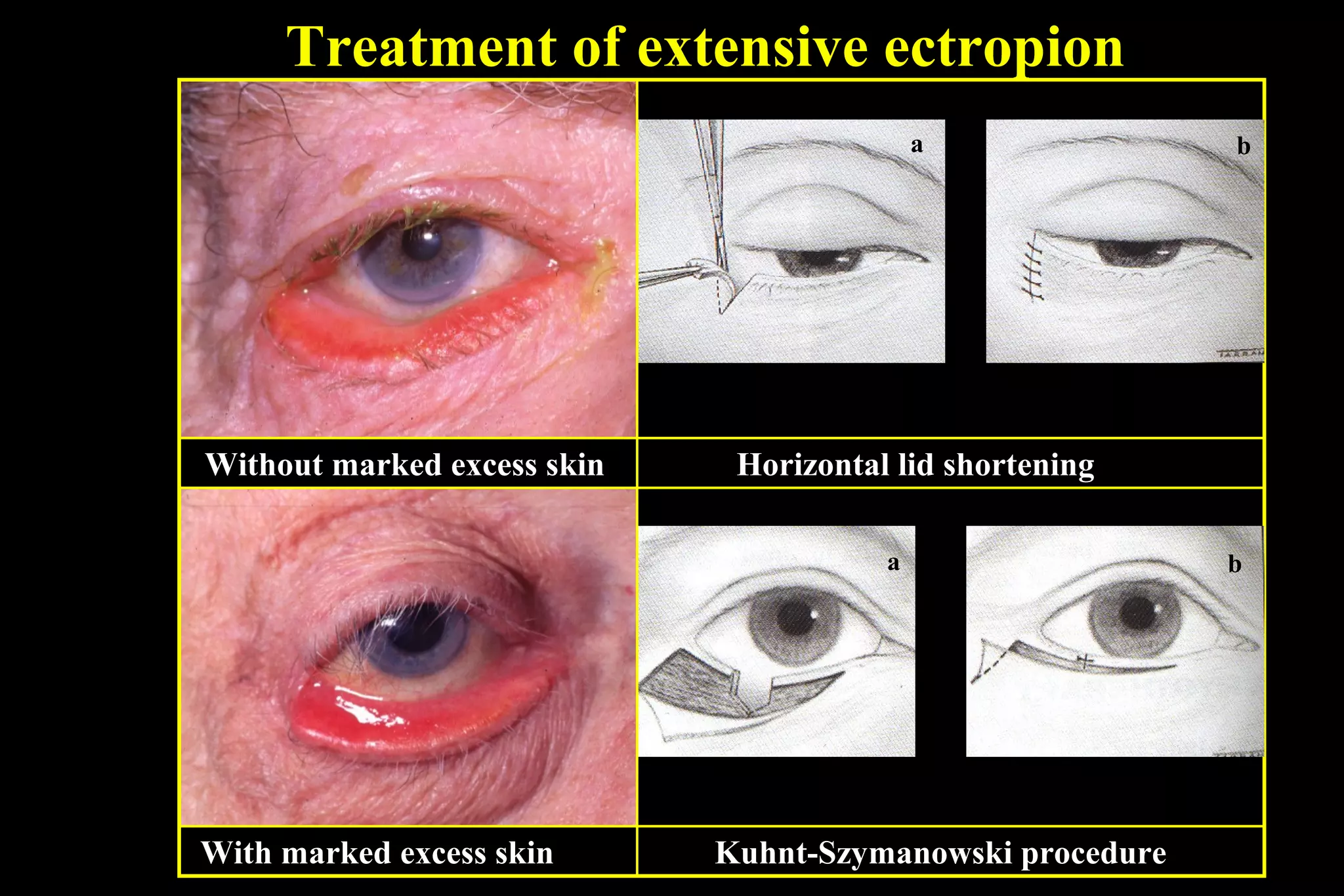
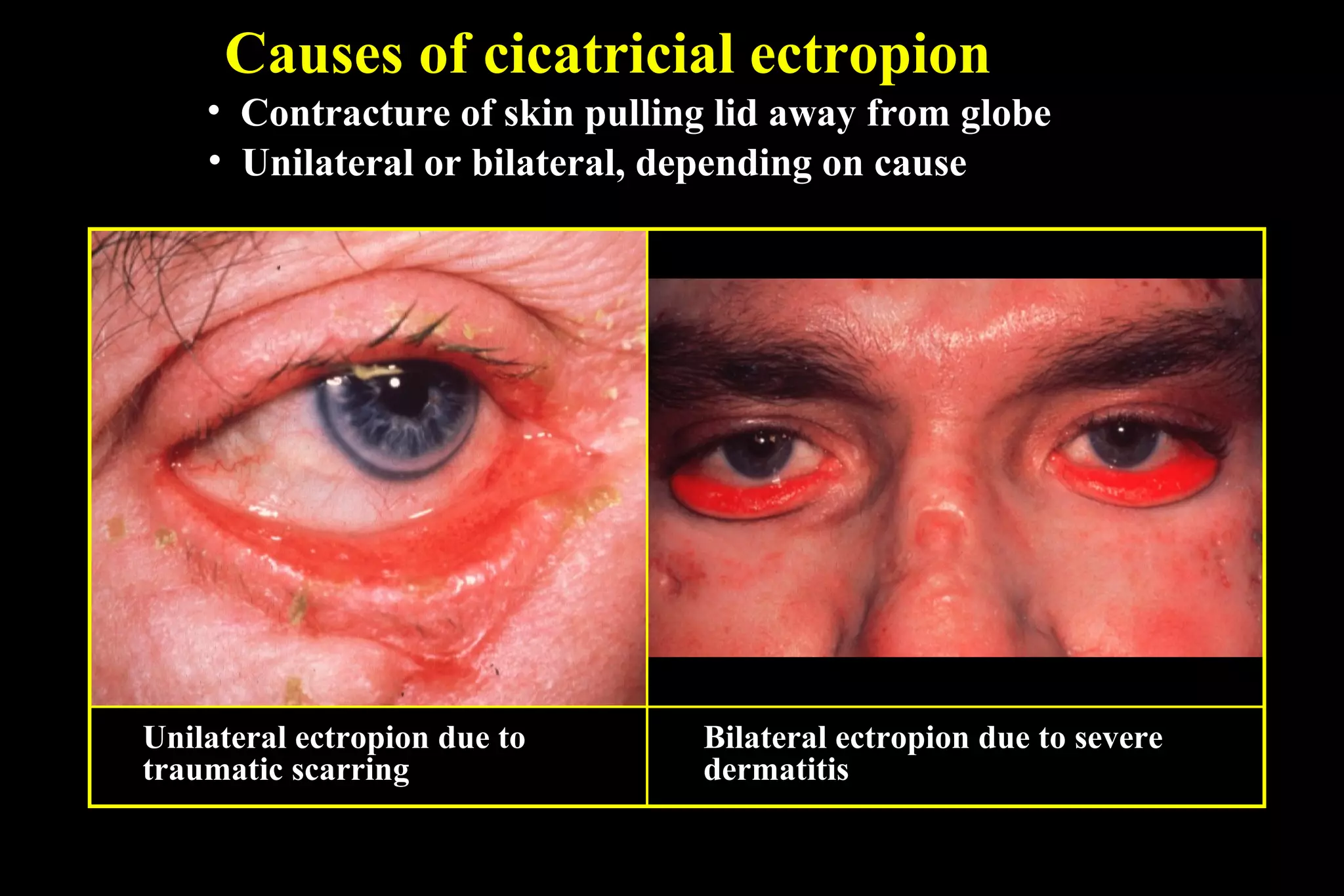
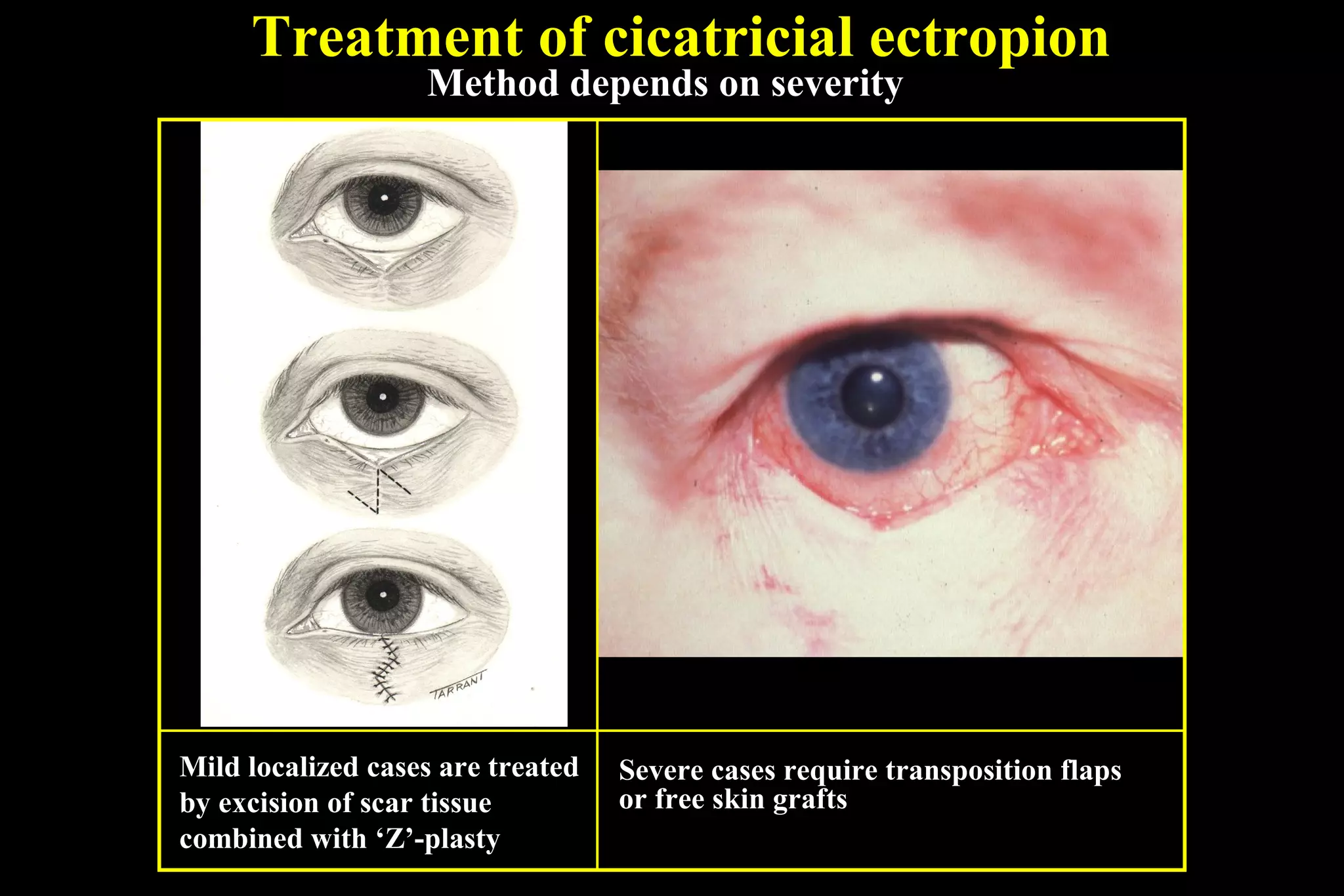
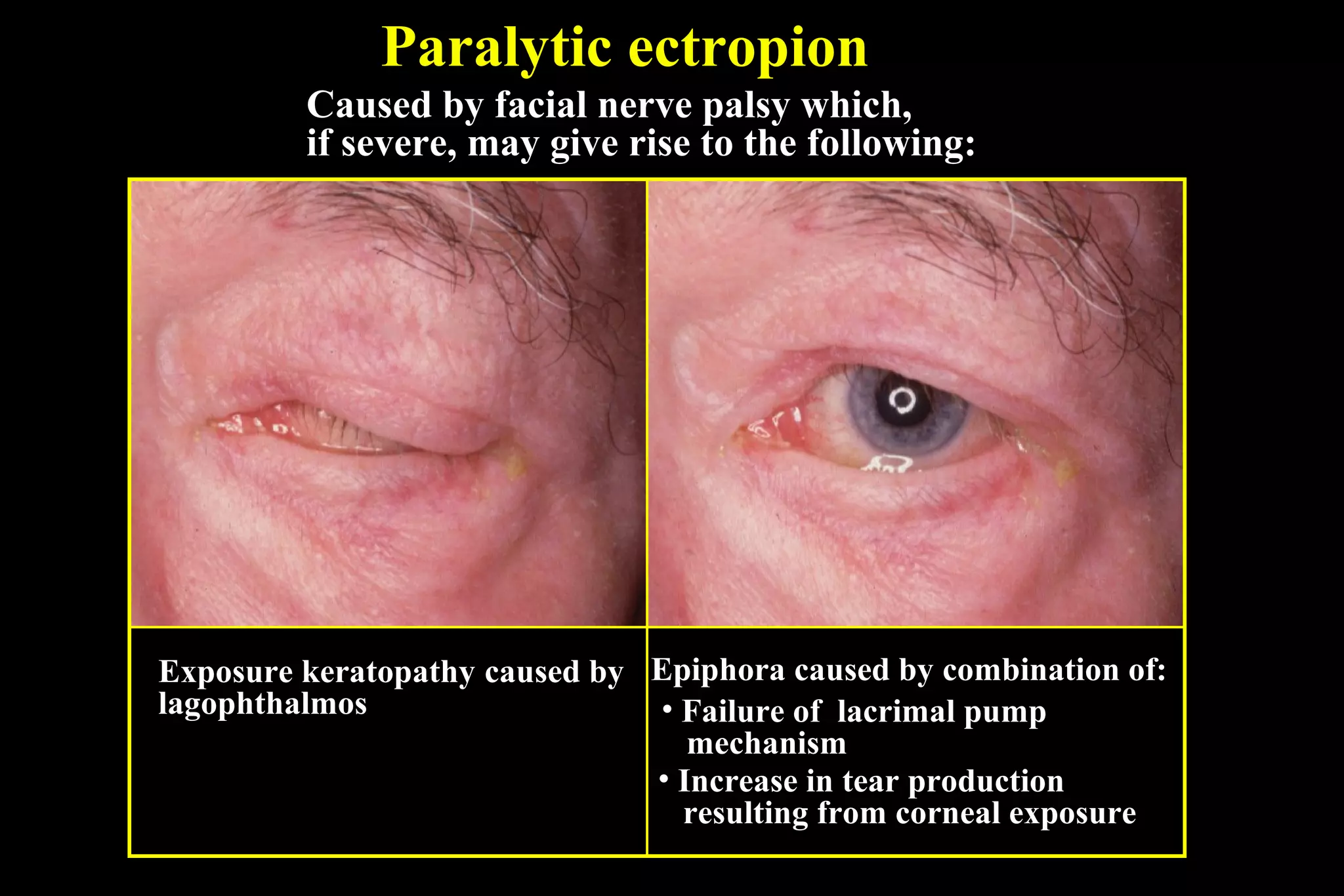
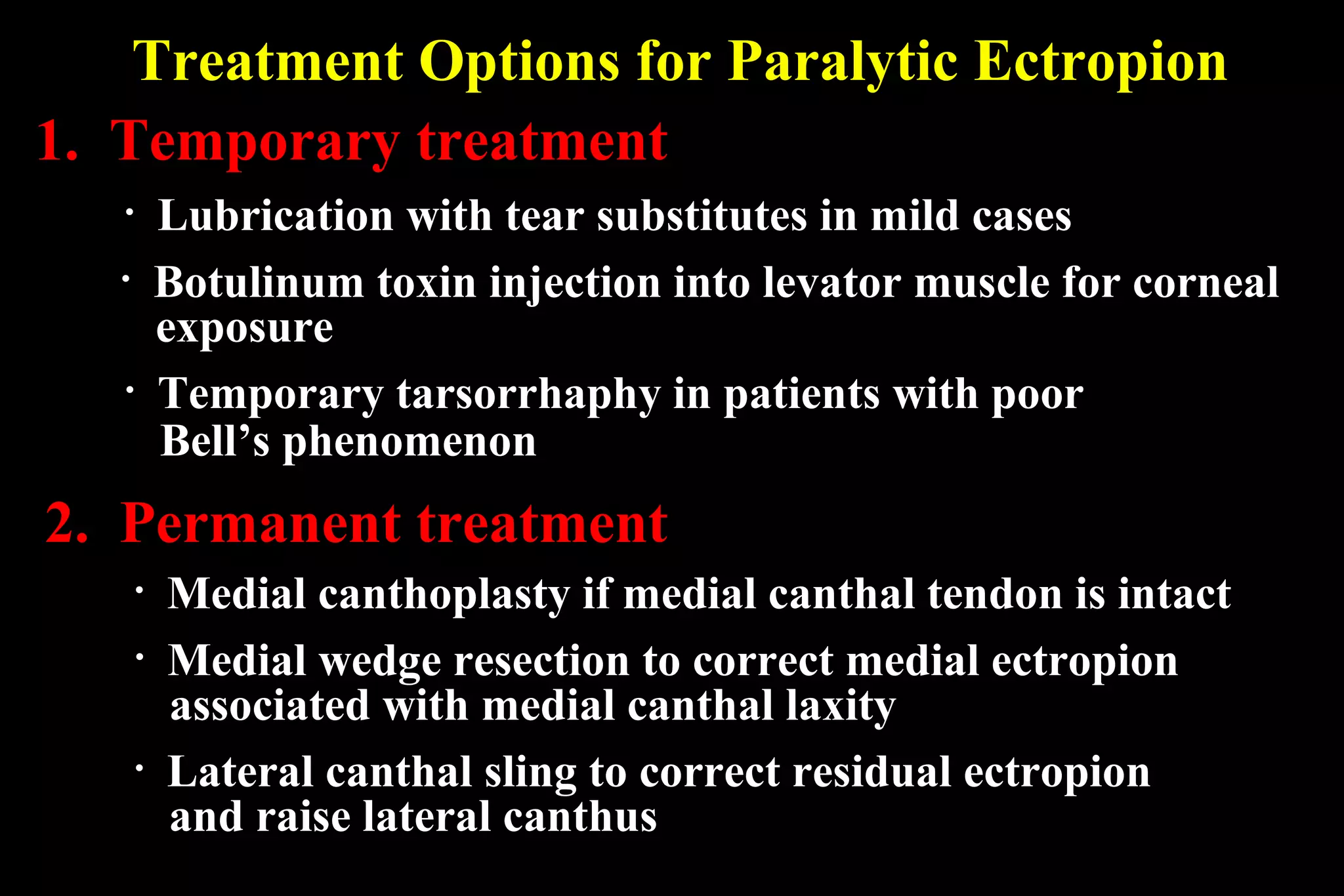
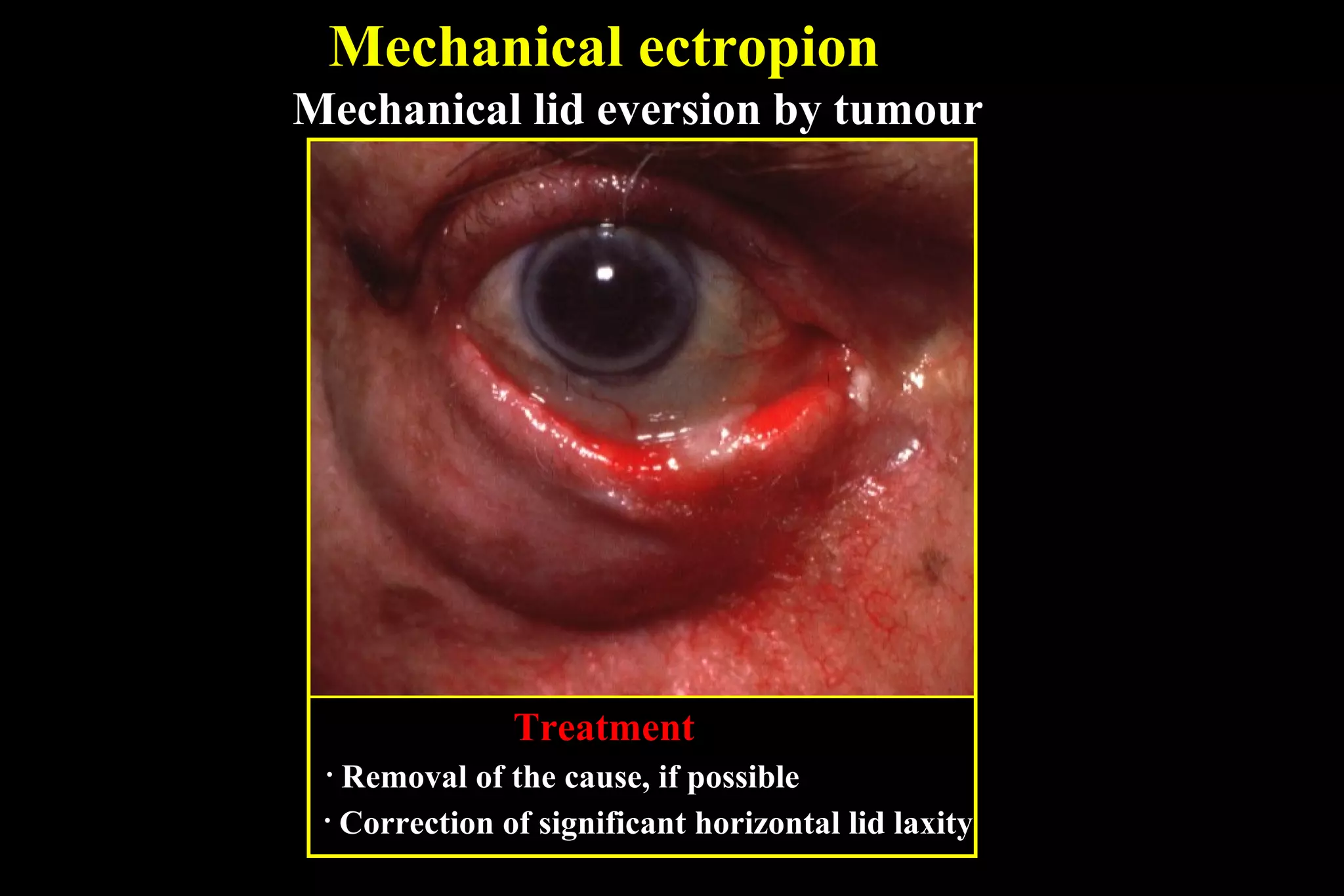
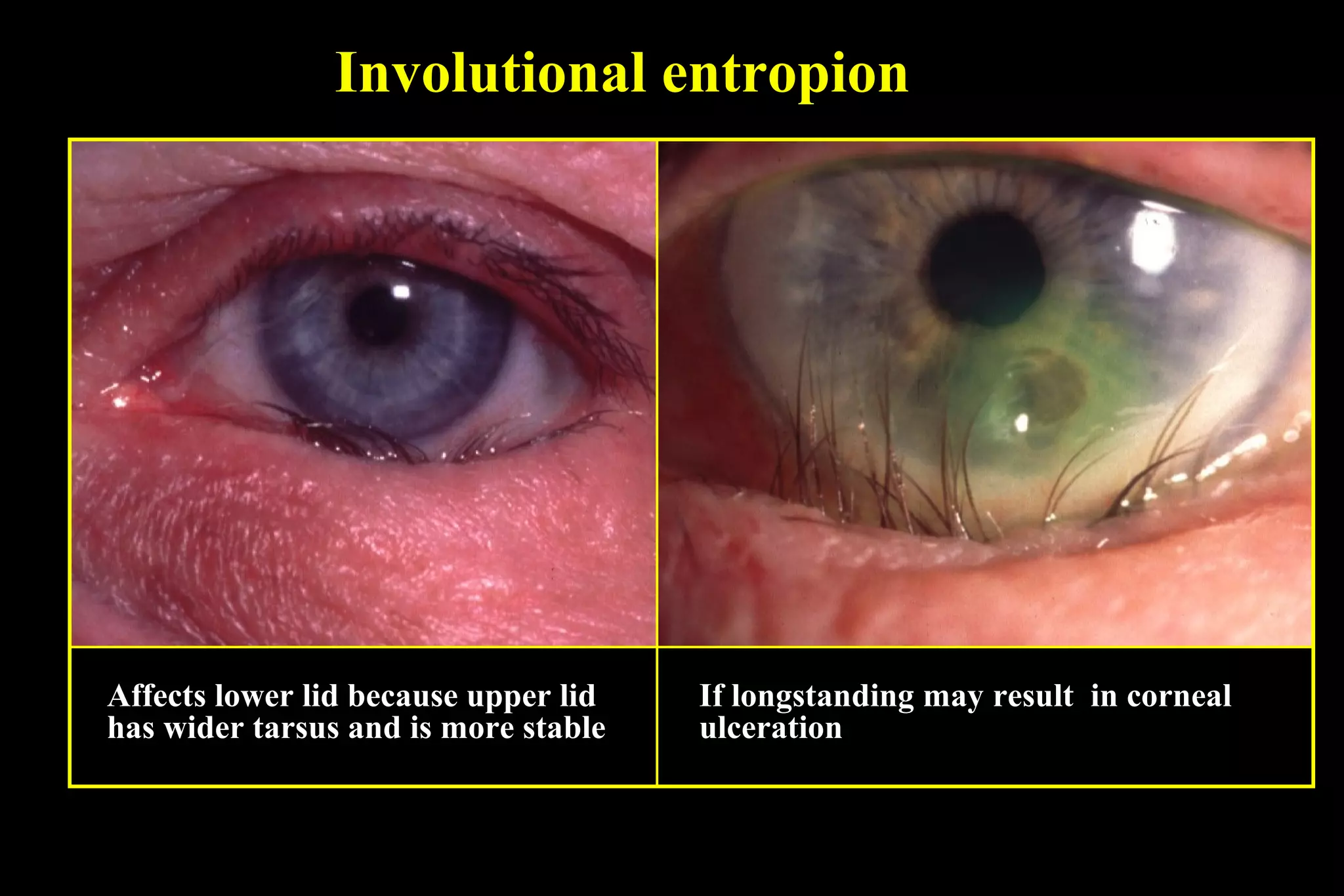
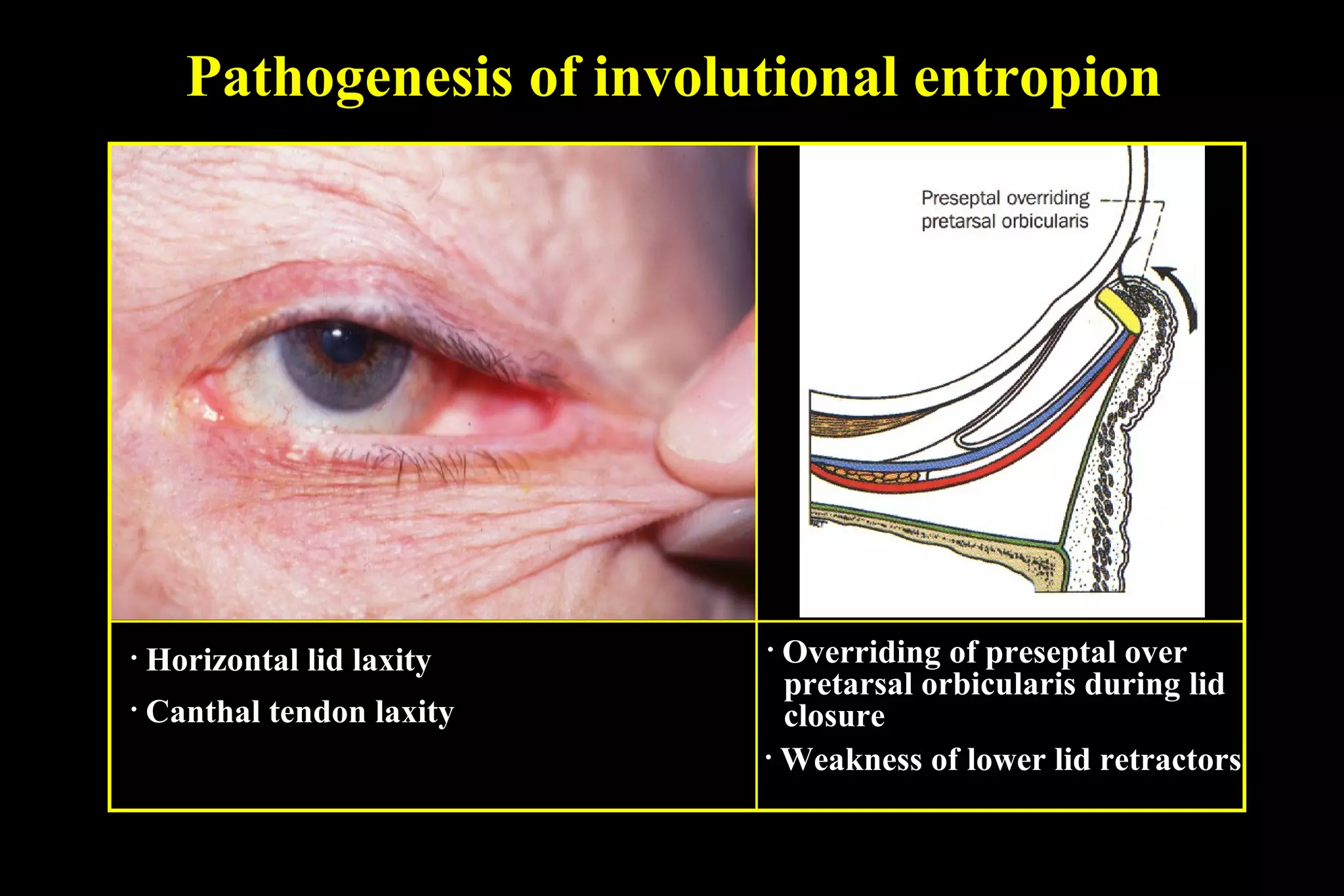
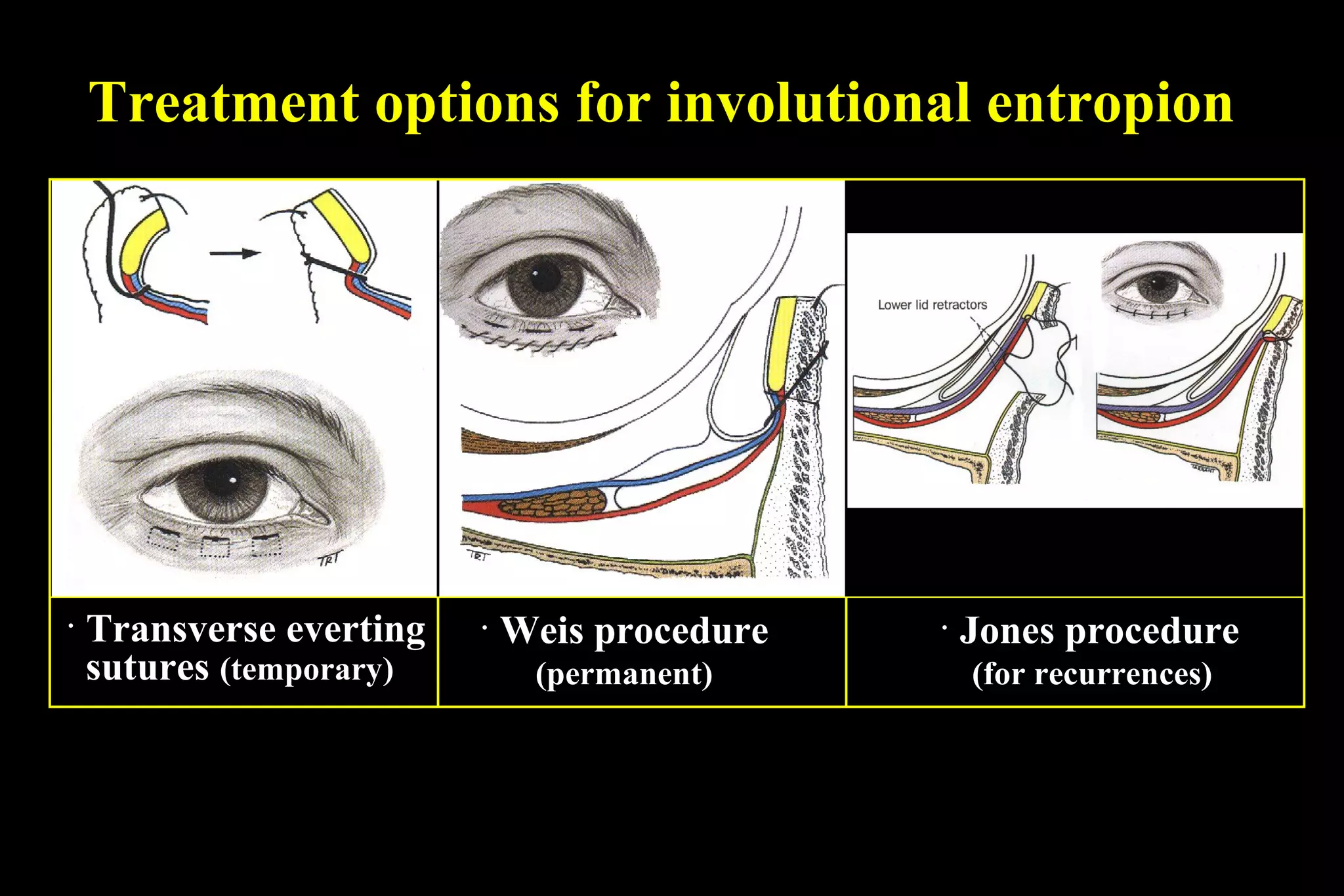
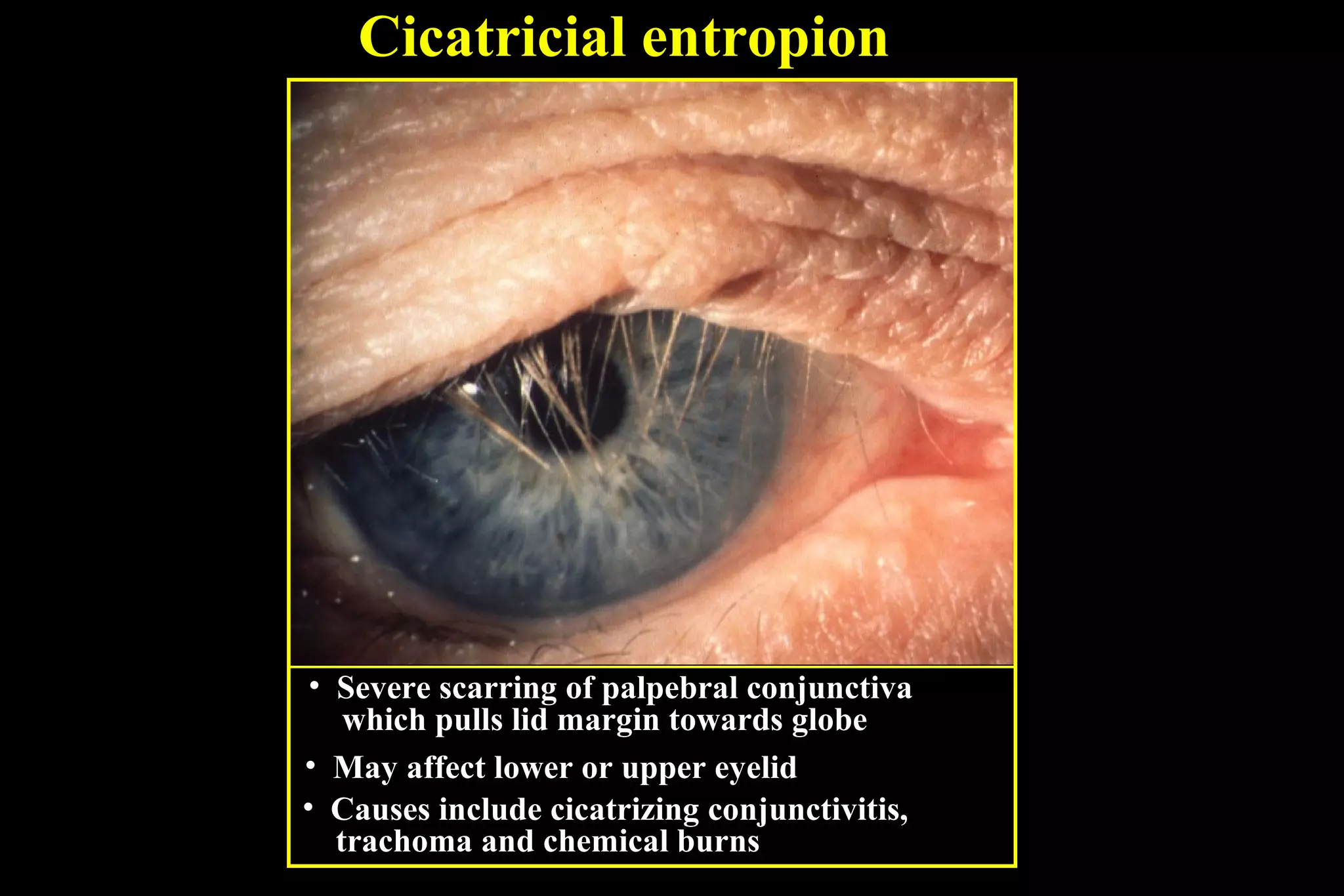
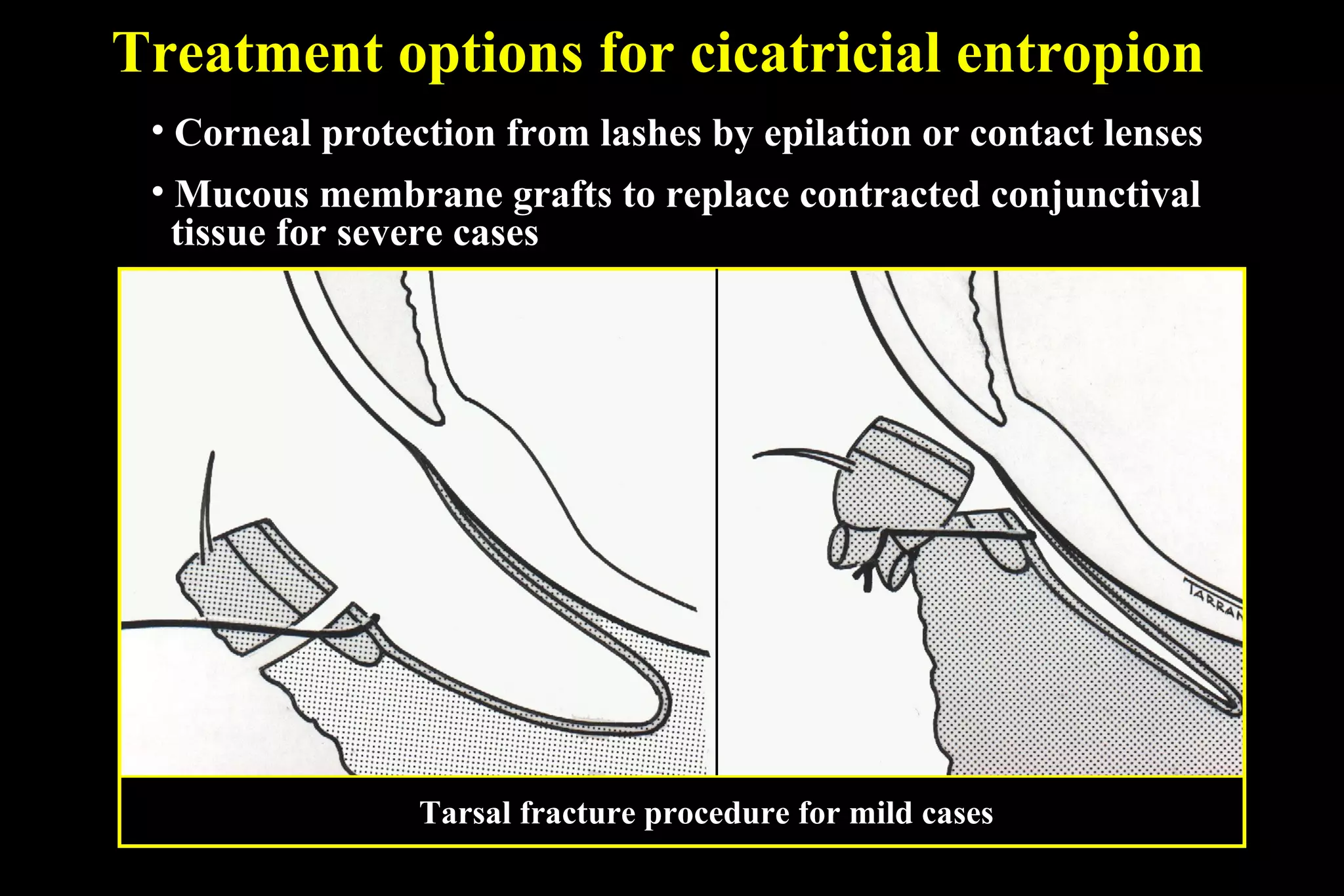
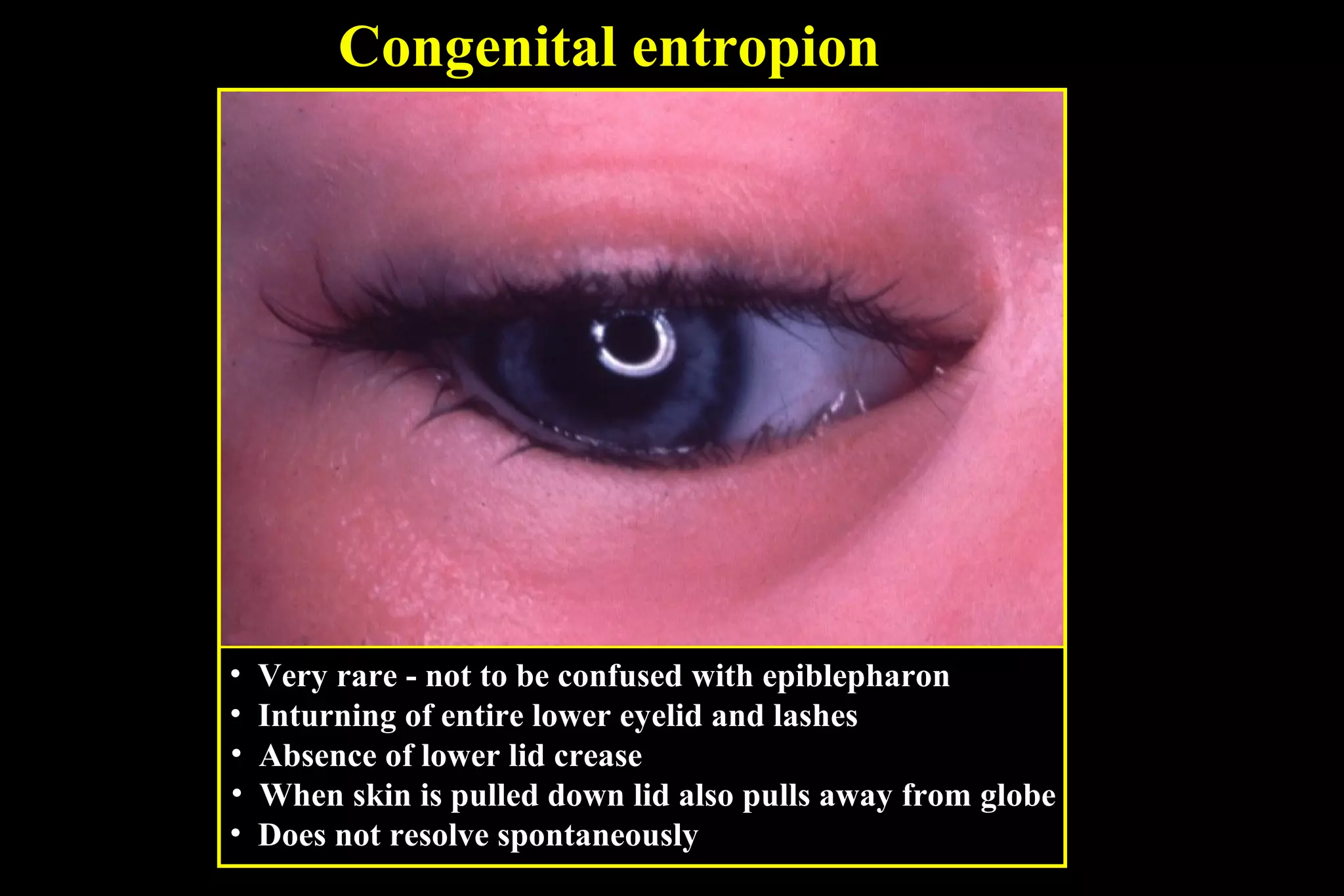

This document describes different types of ectropion and entropion conditions. It discusses involutional, cicatricial, paralytic, congenital, and mechanical causes. Treatment options are provided depending on the severity and include procedures like conjunctivoplasty, wedge resection, tarsorrhaphy, and skin grafts. Assessment of horizontal lid laxity and canthal tendon positioning helps determine the best surgical approach.



























































