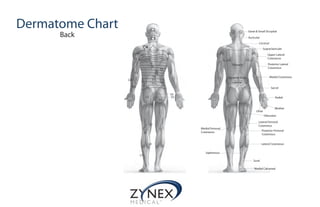
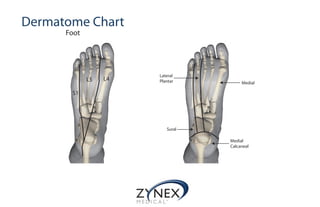
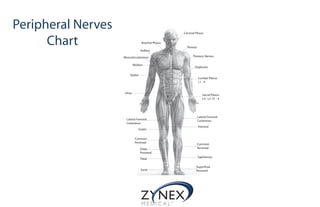
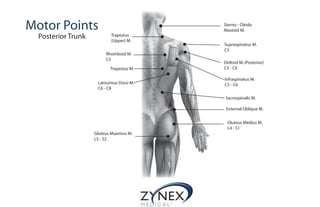
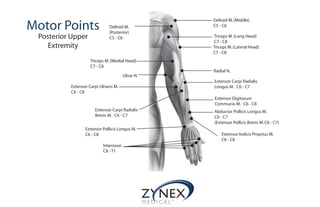
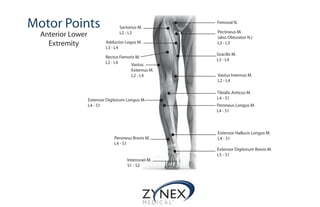
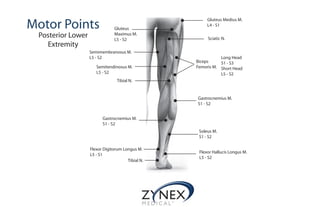
This document contains information about dermatome charts, peripheral nerve charts, and motor point locations for electrostimulation therapy. The dermatome charts show the cutaneous nerve innervation patterns for the front, back, and foot. The peripheral nerve charts display the branches of the cervical, brachial, lumbar, and sacral plexuses. The motor point sections provide diagrams of the anterior and posterior muscle motor points for the trunk, upper extremities, and lower extremities.