Downloaded 71 times






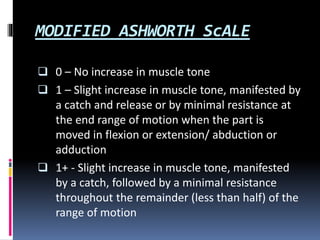
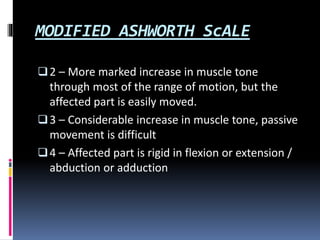





Spasticity is defined as a velocity-dependent increase in muscle tone and exaggerated tendon reflexes caused by hyperexcitability of the stretch reflex. It results from an upper motor neuron lesion and can occur in conditions like spinal cord injury, multiple sclerosis, and cerebral palsy. Spasticity is classified based on severity from mild to severe and causes increasing tightness, spasms, and loss of functional abilities. Treatment involves pharmacological management with drugs like baclofen, physical therapy including stretching and range of motion exercises, and in severe cases surgery such as baclofen pump implantation or tendon lengthening.





















































































