Download to read offline


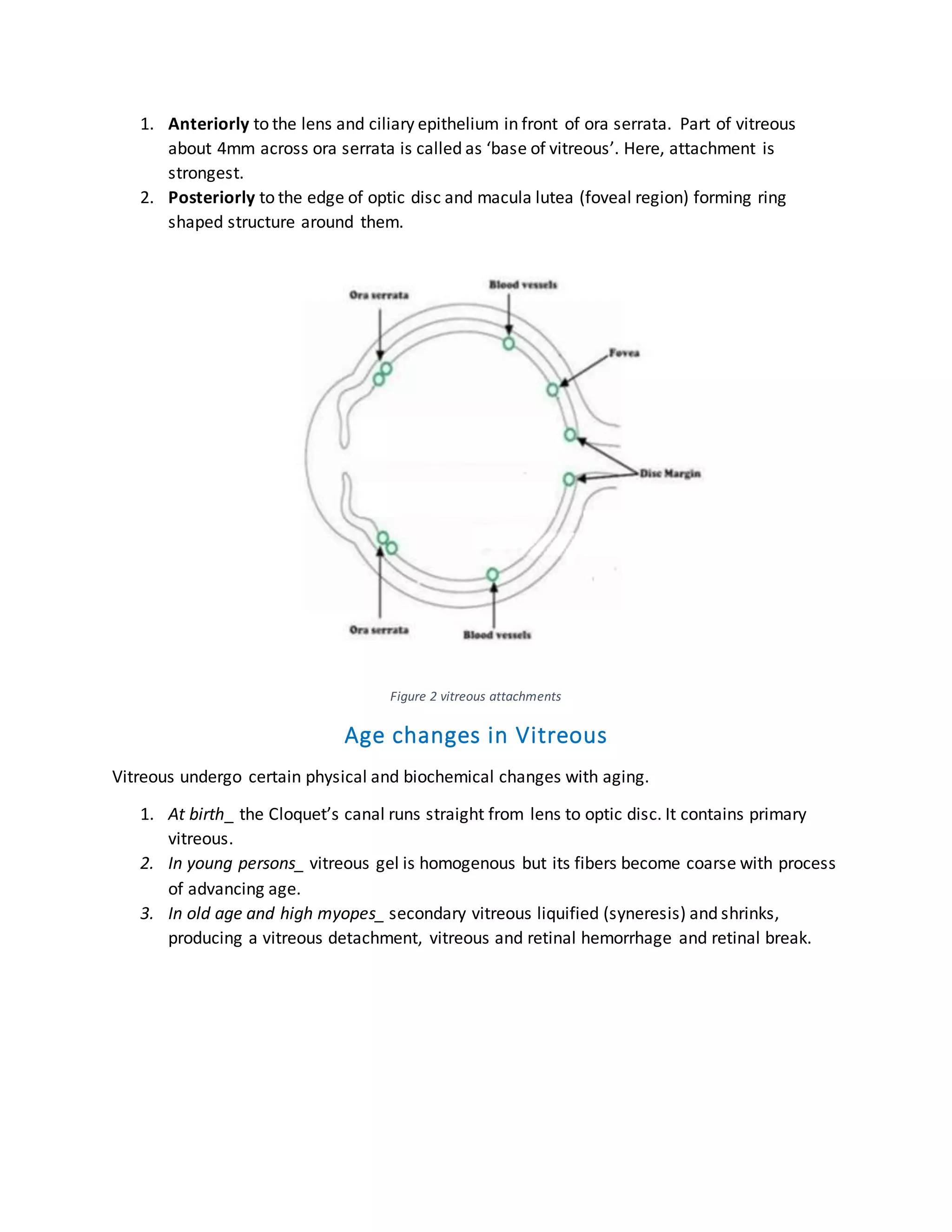
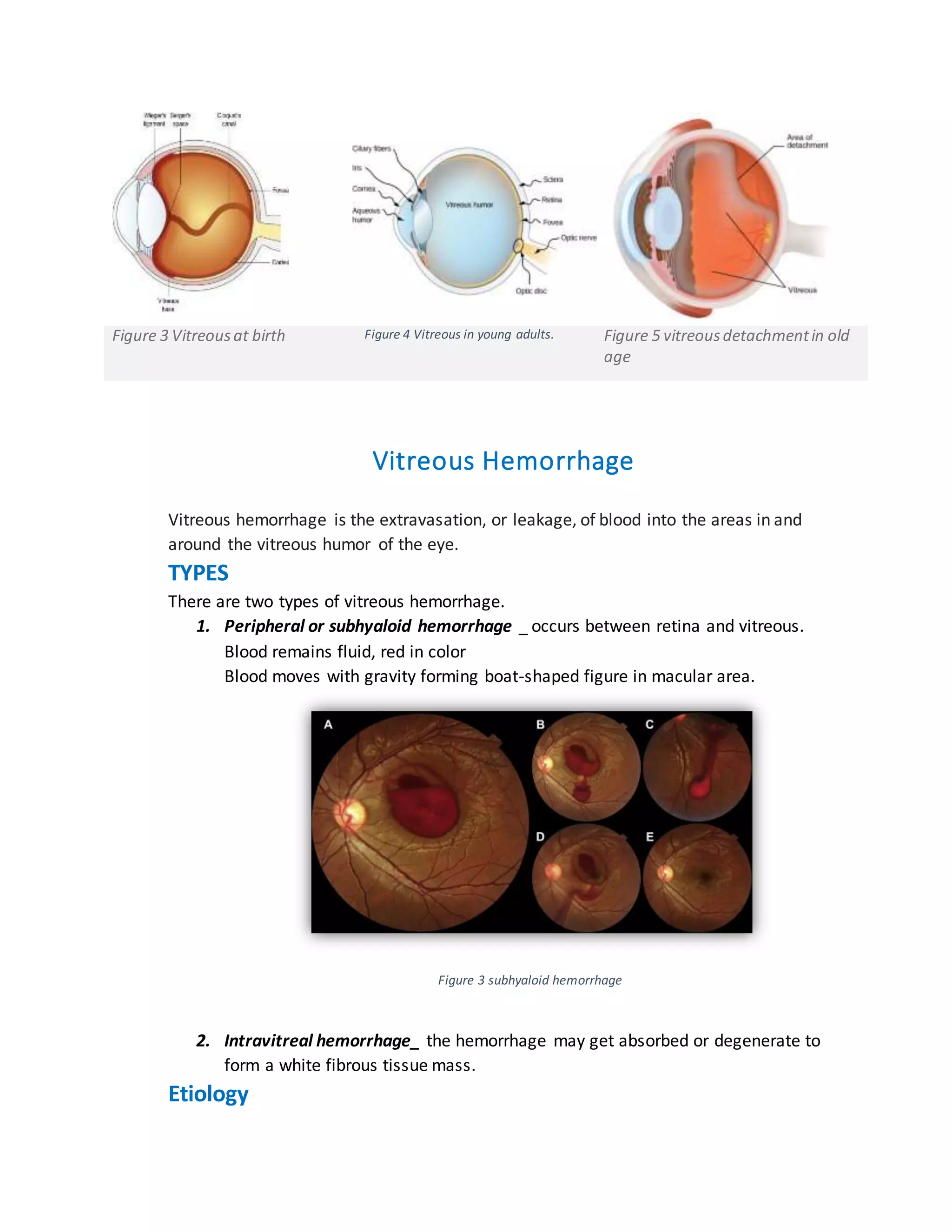

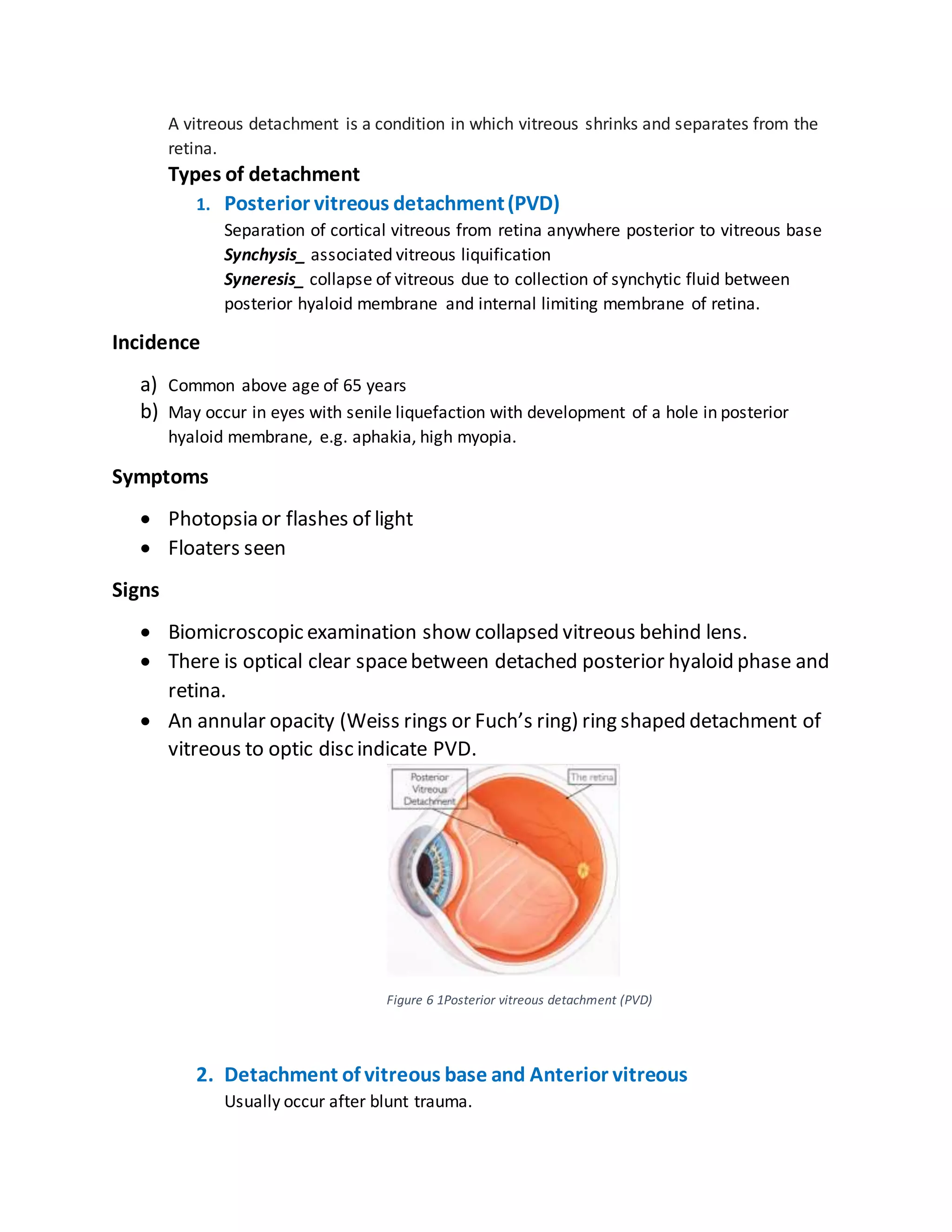




The document provides an overview of vitreous humor, including its structure, functions, and changes with aging, such as liquefaction and detachment. It discusses vitreous hemorrhage types, causes, symptoms, and clinical examination findings. Additionally, it covers posterior vitreous detachment, its symptoms, and its incidence, particularly in individuals over 65 years of age.