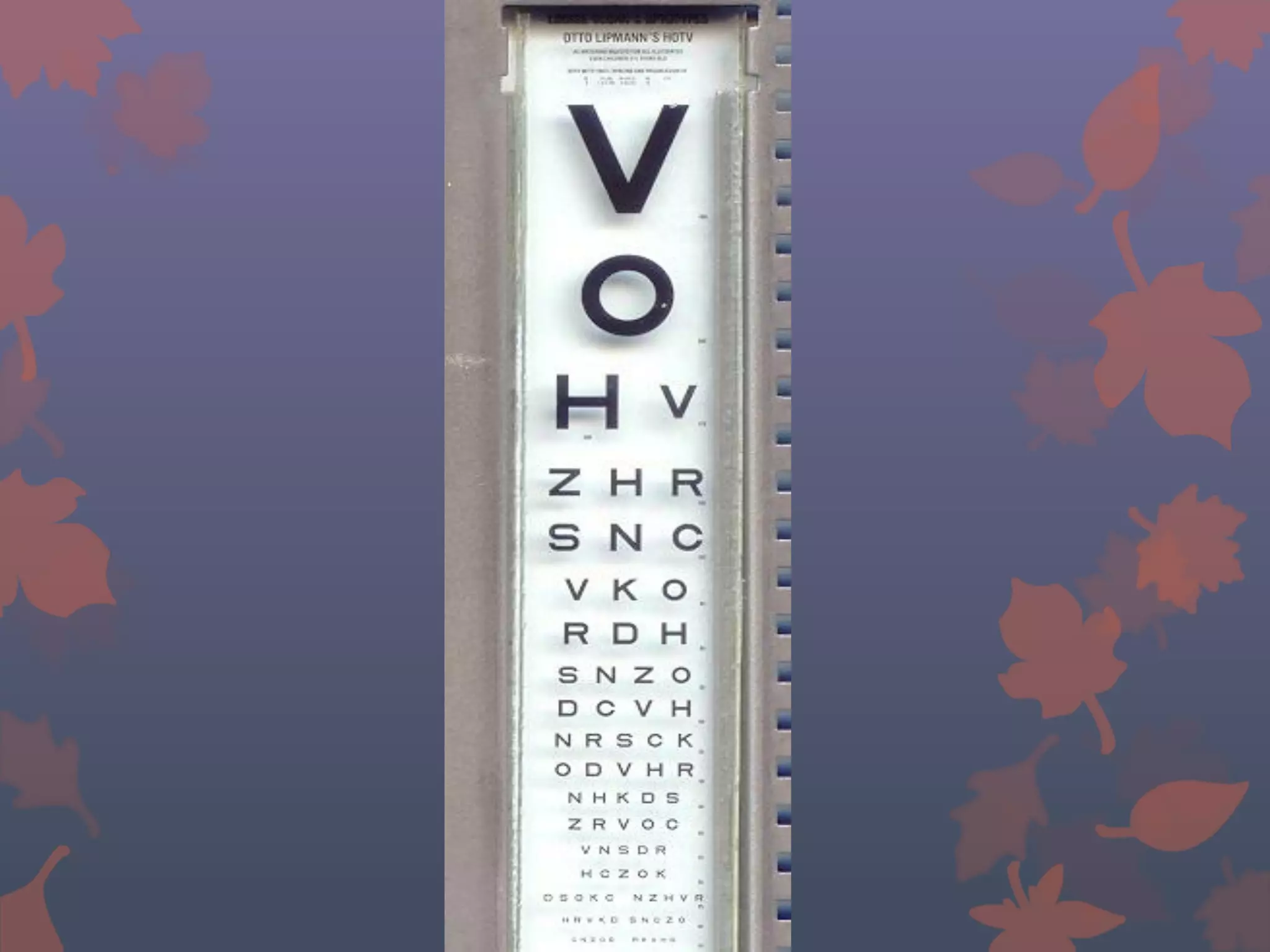
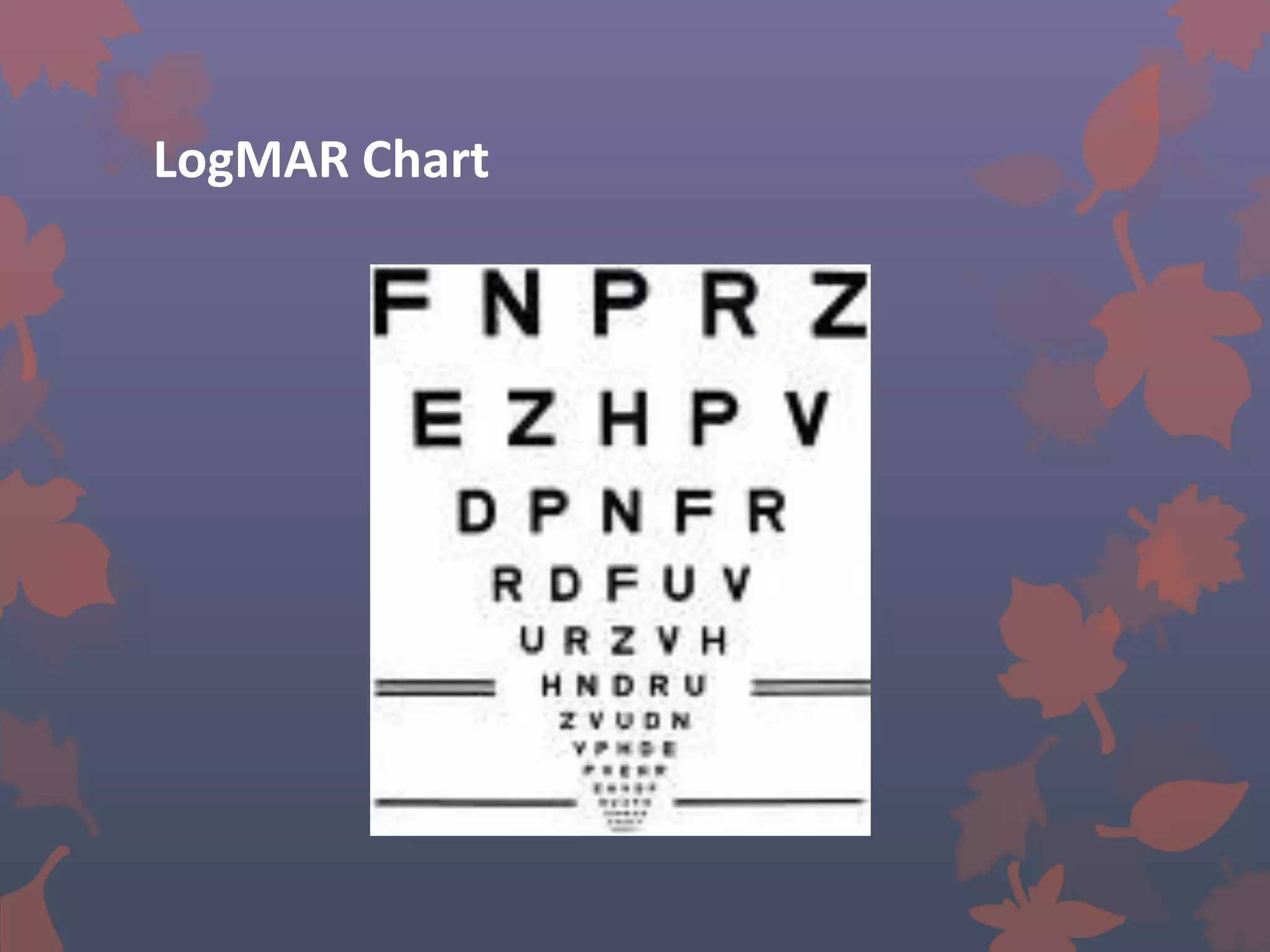
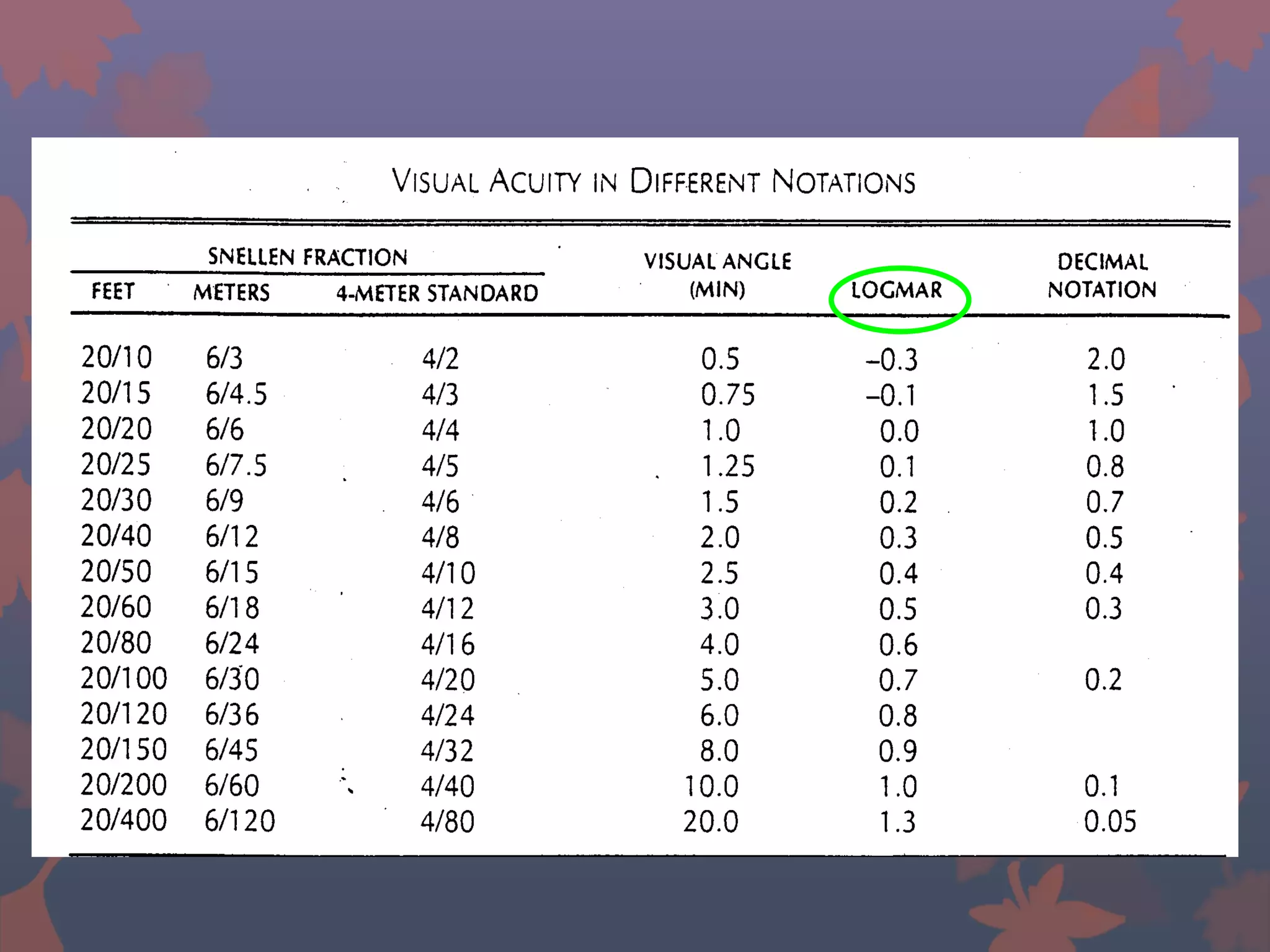
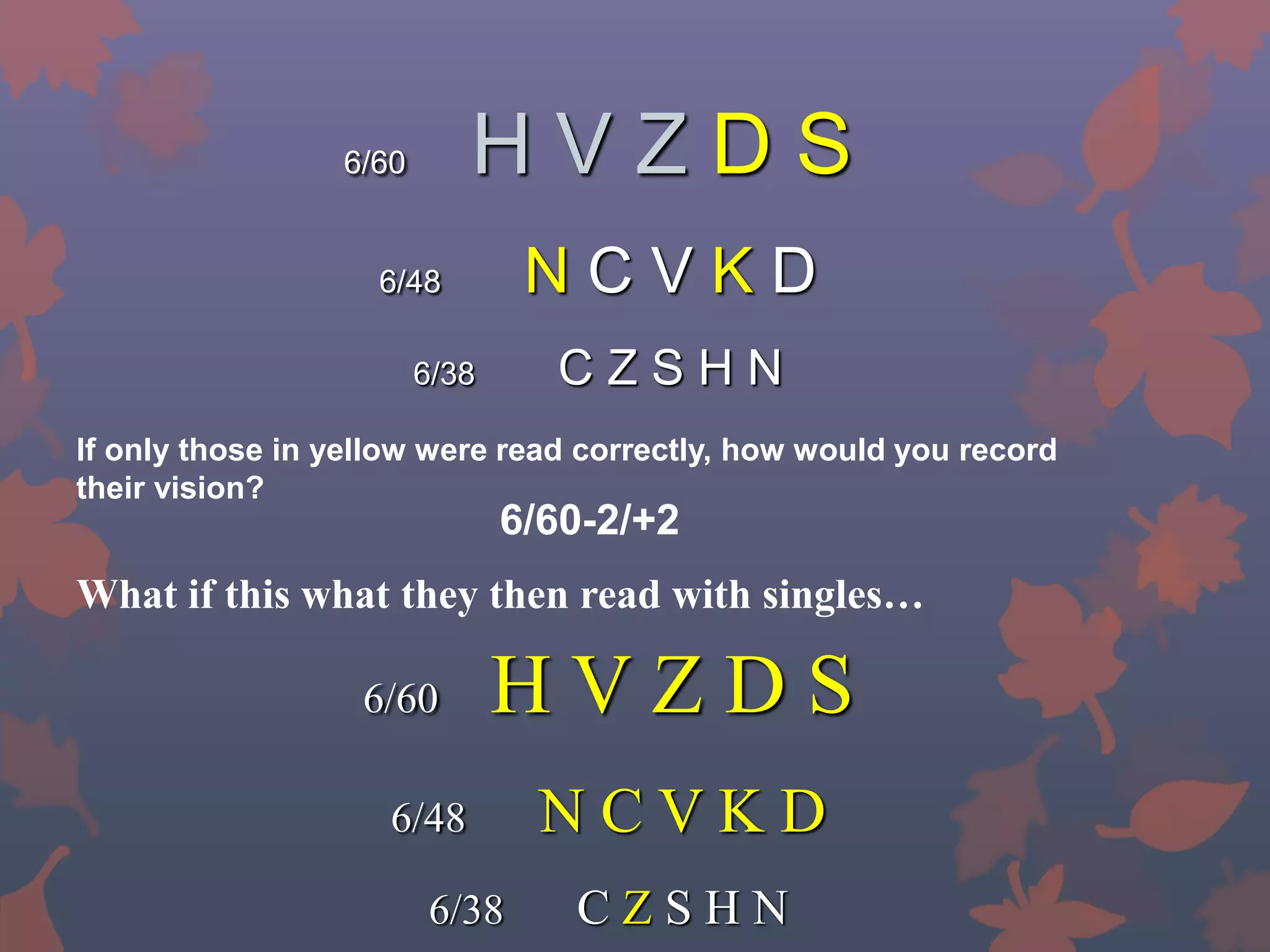
This document provides information on visual acuity assessment. It discusses the different components assessed, including visual acuity, contrast sensitivity, visual fields, and more. It describes the four types of visual perception and defines visual acuity as the spatial limit of visual discrimination, measured as the minimum resolvable angle. The document outlines the different types of visual acuity that can be measured, such as minimum visible acuity, minimum separable acuity, Vernier acuity, and recognition acuity. It also discusses various visual acuity charts, including Snellen, LogMAR, Landolt rings, and preferential looking tests that can be used with infants and young children.