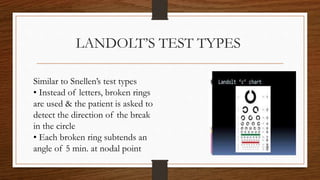
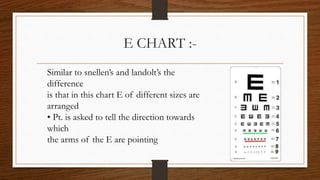
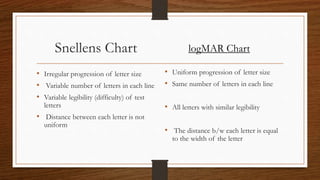
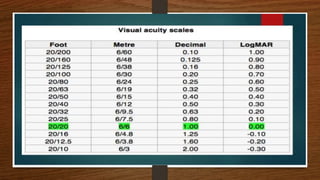
The lecture by Dr. Sania Aslam discusses visual acuity measurement and contrast sensitivity, explaining the principles and clinical tests used to assess visual acuity, including Snellen's test, Landolt's test, and near vision tests. It details the components of visual acuity such as detection, resolution, and recognition, along with methods for testing both adults and children. Additionally, it highlights how visual acuity is expressed in various grading systems like Decimal Acuity and LogMAR.