Download to read offline
![ASSISTANT PROESSOR, s.Y M.SC NURSING, J.G COLLEGE OF
NURSING, J.G COLLEGE OF NURSING,
AHMEDABAD. AHMEDABAD.
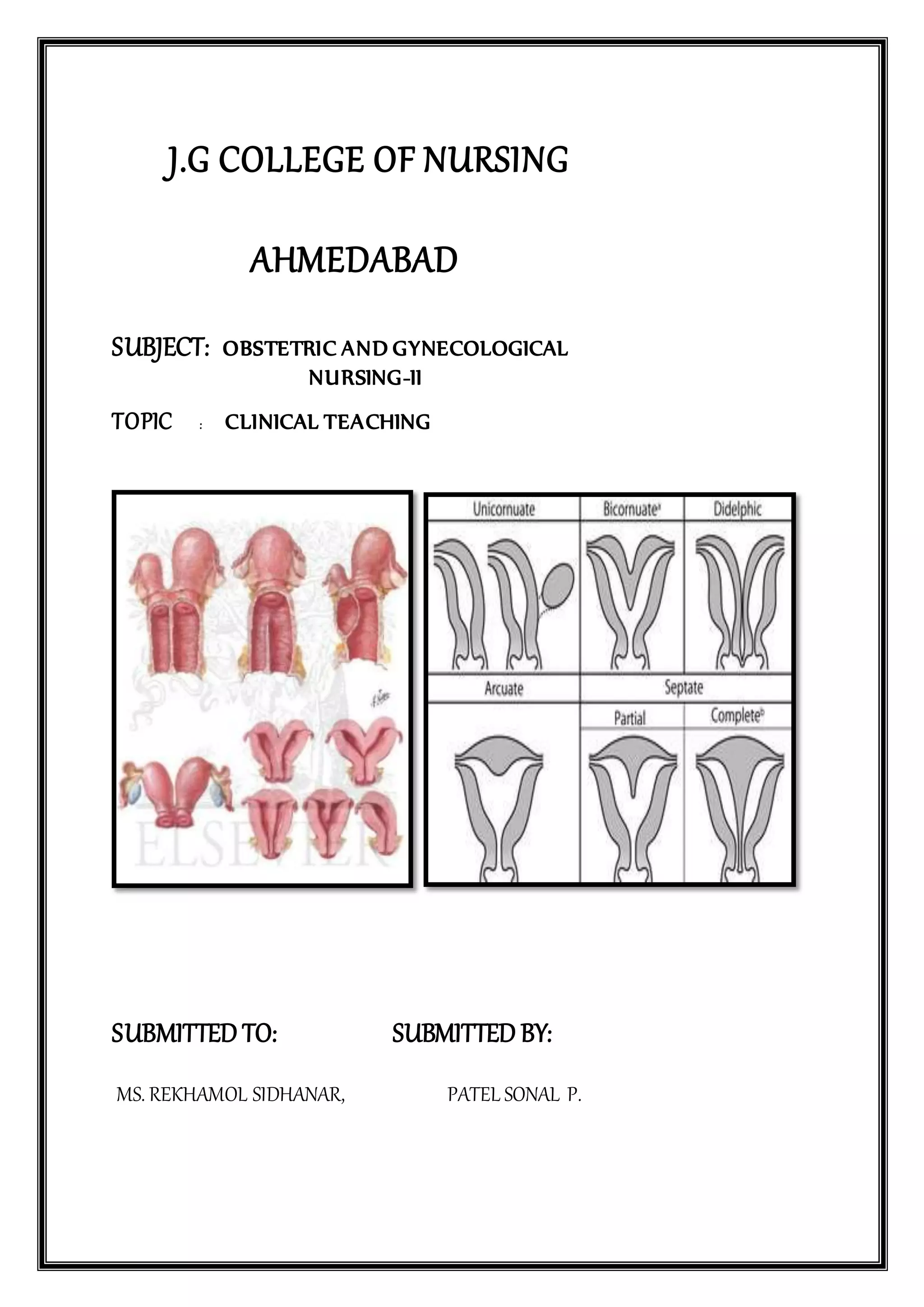
UTERINE MALFORMATION
A uterine malformation is a type of female genital malformation resulting from an
abnormal development of the Müllerian duct during embryogenesis. Symptoms range
from amenorrhea, infertility, recurrent pregnancy loss, and pain, to normal functioning depending on
the nature of the defect.
Prevalence
The prevalence of uterine malformation is estimated to be 6.7% in the general population,
slightly higher (7.3%) in the infertility population, and significantly higher in a population of women
with a history of recurrent miscarriages (16%).[1]
Types
The American Fertility Society (now American Society of Reproductive Medicine) Classification
distinguishes:
Class I: Müllerian agenesis (absent uterus).
Uterus is not present, vagina only rudimentary or absent. The condition is also called Mayer-
Rokitansky-Kuster-Hauser syndrome. The patient with MRKH syndrome will have
primary amenorrhea.
Class II: Unicornuate uterus (a one-sided uterus).
Only one side of the Müllerian duct forms. The uterus has a typical "penis shape" on imaging systems.
Class III: Uterus didelphys, also uterus didelphis (double uterus).
Both Müllerian ducts develop but fail to fuse, thus the patient has a "double uterus". This may be a
condition with a double cervix and a vaginal partition (v.i.), or the lower Müllerian system fused into](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-2-2048.jpg)
![its unpaired condition. See Triplet-birth with Uterus didelphys for a case of a woman having
spontaneous birth in both wombs with twins.
Class IV: Bicornuate uterus (uterus with two horns).
Only the upper part of that part of the Müllerian system that forms the uterus fails to fuse, thus the
caudal part of the uterus is normal, the cranial part is bifurcated. The uterus is "heart-shaped".
Class V: Septated uterus (uterine septum or partition).
The two Müllerian ducts have fused, but the partition between them is still present, splitting the
system into two parts. With a complete septum the vagina, cervix and the uterus can be partitioned.
Usually the septum affects only the cranial part of the uterus. A uterine septum is the most common
uterine malformation and a cause formiscarriages. It is diagnosed by medical image techniques, i.e.
ultrasound or an MRI. MRI is considered the preferred modality due to its multiplanar capabilities as
well as its ability to evaluate the uterine contour, junctional zone, and other pelvic anatomy. A
hysterosalpingogram is not considered as useful due to the inability of the technique to evaluate the
exterior contour of the uterus and distinguish between a bicornuate and septate uterus.
A uterine septum can be corrected by hysteroscopic surgery. Hysterosalpingography of a T shaped
uterus.
Class VI: DES uterus.
The uterine cavity has a "T-shape" as a result of fetal exposure to diethylstilbestrol.
An additional variation is the arcuate uterus where there is a concave dimple in the uterine fundus
within the cavity.
A rudimentary uterus is a uterine remnant not connected to cervix and vagina and may be found on
the other side of an unicornuate uterus.
Patients with uterine abnormalities may have associated renal abnormalities including unilateral renal
agenesis.
"Double vagina"
As the vagina is largely derived from the Müllerian ducts, lack of fusion of the two ducts can lead to
the formation of a vaginal duplication and lack of absorption of the wall between the two ducts will
leave a residual septum, leading to a "double vagina". This condition may be associated with a uterus
didelphys or a uterine septum.[3][4][5]
Since the condition is internal and usually asymptomatic, a
person may not be aware of having a "double vagina." If necessary, the partition can be surgically
corrected, however, there is no valid medical reason for such a procedure.
Diagnosis
Besides a physical examination, the physician will need imaging techniques to determine the
character of the malformation: gynecologic ultrasonography, pelvic MRI, orhysterosalpingography. A
hysterosalpingogram is not considered as useful due to the inability of the technique to evaluate the
exterior contour of the uterus and distinguish between a bicornuate and septate uterus. In](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-3-2048.jpg)
![addition, laparoscopy and/or hysteroscopy may be indicated. In some patients
the vaginal development may be affected.
Treatment
Surgical intervention depends on the extent of the individual problem. With a didelphic uterus surgery
is not usually recommended. A uterine septum can be resected in a simple out-patient procedure that
combines laparoscopy and hysteroscopy. This procedure greatly decreases the rate of miscarriage for
women with this anomaly.
Congenital Uterine Anomalies
The true incidence of congenital uterine anomalies in the general population and among women with
RPL is not known accurately. Although incidences of 0.16 to 10% have been reported, the overall
data suggest an incidence of 1% in the general population and 3% in women with RPL and poor
reproductive outcomes. In a comparative study of women with and without a history of RPL using
three-dimensional ultrasound, Salim et al found major congenial anomalies in 6.9% of women with
RPL compared with 1.7% in low-risk women. Overall, the prevalence of major congenital anomalies
appears to be three-fold higher in women with RPL compared with women without a history of
recurrent miscarriage.
Many nonobstructing uterine abnormalities are asymptomatic and may be discovered only in the
evaluation of RPL, persistent menstrual irregularities, or infertility. Additional complicating matters
include the lack of uniform imaging modalities for diagnosis.
Müllerian Development
Sexual differentiation begins early in the fetal period. Up until the sixth week of life the male and
female genital systems are identical. There are two pairs of symmetrical genital ducts, the
mesonephric (Wolffian) duct and the paramesonephric (müllerian) ducts. The müllerian ducts arise as
coelomic invaginations in the mesonephros, and their formation is thought to be induced by the
mesonephric duct. In the female embryo, in the absence of fetal testes, testosterone, and müllerian-
inhibiting substance, the Wolffian ducts begin to degenerate and allow for the maturation of the
müllerian ducts. The müllerian ducts grow caudally and become enclosed in peritoneal folds that later
give rise to the broad ligaments of the uterus, to which the ovaries (mesovarium), fallopian tubes
(mesosalpinx), and uterus (mesometrium) are attached. The müllerian ducts approach each other and
begin to fuse. At 9 weeks gestation, the septum from the fused ducts begin to resorb, forming a tube
with a single lumen called the uterovaginal canal. This becomes the uterus and upper portion of the
vagina, whereas the unfused cranial portions of the müllerian ducts become the fallopian tubes. The
lower portion of the vagina is formed from the sinovaginal bulb of the urogenital sinus. The
uterovaginal canal elongates to eventually unite with the urogenital sinus, thus forming the
completion of the female reproductive tract.
Müllerian tract anomalies result from failure to complete bilateral duct elongation, fusion,
canalization, or septal resorption of the müllerian ducts. They may occur in any step during this
developmental process. The etiologies of such disorders are still widely unknown.
Classification
In an effort to describe the diverse müllerian anomalies encountered, Buttram and Gibbons[12]
in 1979
grouped the anomalies according to their clinical morphology. This was later modified in 1988 by the
American Fertility Society (currently known as the America Society for Reproductive Medicine) and
is now the most commonly accepted means of characterizing müllerian tract defects.
The American Society for Reproductive Medicine classification of müllerian anomalies. *Uterus may
be normal or take a variety of abnormal forms. **May have two distinct cervices. DES,
diethylstilbestrol. (From Anonymous. The American Fertility Society classifications of adnexal
adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies,
müllerian anomalies and intrauterine adhesions. Fertil Steril 1988;49(6):944–955.](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-4-2048.jpg)
![ Class I: Müllerian agenesis or hypoplasia
Class II: Unicornuate uterus
Class III: Didelphys uterus
Class IV: Bicornuate uterus
Class V: Septate uterus
Class VI: Arcuate uterus
Class VII: Diethylstilbestrol (DES)-exposed uterus
UTERINE SEPTUM
The septate uterus is a result of absent or incomplete resorption of the intervening
uterovaginal septum following fusion of the müllerian ducts. It is the most common congenital
anomaly of the uterus, comprising approximately 55% of all anomalies. A septum is primarily
composed of fibromuscular tissue that may project minimally from the uterine fundus or may extend
to the cervical os, almost completely dividing the uterine cavity in two. Septa also may be segmental,
resulting in partial communications between the two sides.
Fedele used scanning electron microscopy to compare endometrial biopsy specimens obtained
from the septum and the lateral uterine wall in the preovulatory phase. They found that the septal
endometrium showed defective development, indicative of a reduction in sensitivity to steroid
hormones. This suggests that there may be local defects that interrupt normal early embryo
development after implantation, resulting in first-trimester miscarriage.
Surgical intervention should be considered when a septate uterus is found in association with
adverse reproductive outcome. Most studies evaluating the efficacy of metroplasty are observational,
retrospective, and include small sample sizes, and therefore are not ideal. However, they seem to
indicate that reproductive outcomes are improved after hysteroscopic resection. Fedele evaluated the
reproductive outcome after hysteroscopic metroplasty in 31 women with infertility and 71 women
with miscarriage, and reported a cumulative pregnancy rate of 89% at 36 months for patients with
complete septum and 80% for those with partial septum. The overall miscarriage rate was 15%.
Homer et al[6]
reviewed the reproductive outcome before and after hysteroscopic metroplasty in
published series and showed a dramatic decrease in the overall miscarriage rate from 88% to
approximately 15% after surgery.
Hysteroscopic septal incision is now the preferred method for treatment of the septate
uterus.[6]
The technique involves incision of the septum between the anterior and posterior uterine
walls extending up to the fundus but not into the fundal myometrium. Hysteroscopic septal incision
can be performed using microscissors, electrosurgery, or fiberoptic laser energy. A theoretical
advantage of scissors over electrosurgery or laser is that there is no risk of thermal myometrial
vascular damage, which may predispose to intrauterine synechiae. Thick septa, however, may be
easier to incise with an electrical technique than with the scissors. In addition, hemostasis is easily
achieved at the same time with use of coagulation current. Although lasers have the advantage of](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-5-2048.jpg)
![speed and good hemostasis, they are expensive and usually more difficult to
manipulate. Transabdominal metroplasty has been used in the past but has been abandoned because of
the higher risk of complications, including postoperative reduction of intrauterine volume, formation
of intrauterine and pelvic adhesions, and tubal occlusion.
Laparoscopic guidance frequently is used during hysteroscopic metroplasty to reduce the risk
of uterine perforation. It also allows the surgeon to differentiate accurately between a septate and
bicornuate uterus. Ultrasonographic guidance has been suggested for difficult cases where
laparoscopy is contraindicated.
UNICORNUATE UTERUS
Agenesis or hypoplasia of one of the müllerian ducts results in the unicornuate uterus arising
in approximately 20% of uterine anomalies.[14]
There are many variations of this anomaly. The
functional uterus may exist alone or may be accompanied by a rudimentary uterine horn. The
rudimentary horn, in turn, may be categorized into groups based on the presence or absence of a
cavity. Further classification is determined by whether or not the uterine horn communicates with the
fully differentiated uterus. If a rudimentary horn is present with a cavity, the patient may present with
unilateral cyclical pelvic pain secondary to hematometra. Associated renal anomalies occur in 40% of
patients (higher than in any other class), and are usually ipsilateral to the hypoplastic horn.
Spontaneous abortion rates in these women approach 51%, premature birth rates approach
15%, and fetal survival is estimated at 39%.Other pregnancy complications include malpresentation,
IUGR, uterine rupture, and ectopic pregnancies. The pathogenesis of pregnancy loss appears to be
related to reduced intraluminal volume and/or inadequate vascular supply to the developing fetus and
placenta. There are no surgical procedures to enlarge the uterus. The higher prevalence of cervical
incompetence in uterine anomalies, however, has led some authors to recommend that cervical
cerclage be placed to improve obstetrical outcome. These are mostly anecdotal reports and small case
series and they report some improvement in obstetrical outcome. However, there are no studies
addressing the prophylactic and empirical use of cervical cerclage. Therefore, based on the current
available evidence, women with a unicornuate uterus and no previous history of second-trimester loss
or premature birth should be managed expectantly with frequent assessment of cervical length and
anatomy. It is recommended that unicornuate uteri with rudimentary horns be resected because of
dysmenorrhea and hematometra as well as the potential for ectopic pregnancy and uterine rupture.
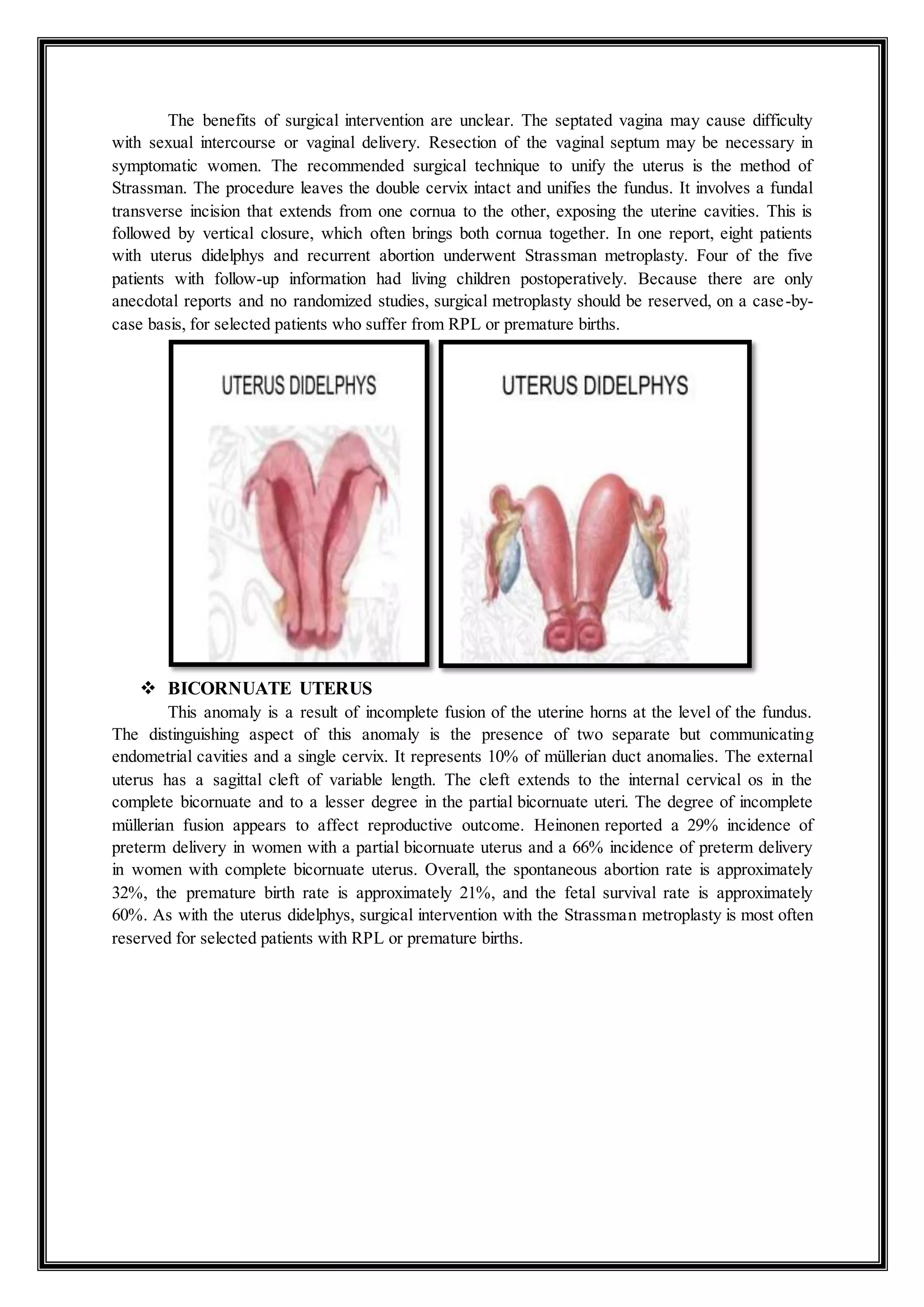
UTERUS DIDELPHYS
In this condition, there is nonobstructed failure of lateral fusion involving both the uterus and
vagina. This results in the formation of a double uterus, double cervix, and double vagina. Uterus
didelphys is one of the least common anomalies, representing approximately 5 to 7% of müllerian
defects.[14]
The reproductive outcomes are slightly better than those of women with unicornuate
uterus. The spontaneous abortion rates are estimated at 43%, the premature birth rate is approximately
38%, and the fetal survival rate is approximately 54%.](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-6-2048.jpg)
![ ARCUATE UTERUS
The near-complete resorption of the uterovaginal septum may leave a mild concave
indentation of the endometrial cavity at the level of the fundus, giving the uterus an arcuate
configuration. It is not clear if this configuration represents a true anomaly or an anatomic variant.
Reproductive outcome data in this condition are conflicting and both positive and negative outcomes
have been reported.[14]
In a retrospective case series of 176 patients, Acien reported a 45% early
abortion rate in women with arcuate uterus. In contrast, Raga et al in their series noted only a 13%
early miscarriage rate in women with this anomaly. Treatment is usually expectant.
DES Exposure
DES is an orally active synthetic estrogen that was introduced in the 1940s for the treatment
of RPL, premature delivery, and other complications of pregnancy. Uterine abnormalities are common
and appear to occur in 69% of women exposed to DES in utero. The most common abnormality is a
T-shaped uterine cavity (70%). Other abnormalities include a small uterus, constriction rings, and
intrauterine filling defects. In addition, 44% of the women have structural changes in the cervix](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-8-2048.jpg)
![including an anterior cervical ridge, cervical collar, cervical hypoplasia, and pseudopolyps. The use of
DES in pregnancy was banned in 1971. Women with a history of in utero exposure to DES appear to
have a greater risk of adverse pregnancy outcome, including a two-fold increased risk of spontaneous
abortion (24% in DES-exposed women versus 13% in controls) and a nine-fold increase in ectopic
pregnancy rates (5% in DES-exposed women compared with 0.5% in controls).
Women with in utero exposure to DES are predisposed to cervical incompetence. In one
nonrandomized study, 63 women with in utero DES exposure were treated with prophylactic cerclage
or expectant management. Eighty-eight percent of women who received cerclage delivered at term
compared with 70% who did not receive a cerclage.[39]
Prophylactic cerclage may be beneficial to
DES-exposed women with history of second-trimester loss or preterm delivery.
BIBLIOGRAPHY
Sotirios H. Saravelos; Karen A. Cocksedge; Tin-Chiu Li (2008). "Prevalence and
diagnosis of congenital uterine anomalies in women with reproductive failure:
ariticalappraisal.". HumanReproductionUpdate. 14 (5):29. PMID 18539641. d
oi:10.1093/humupd/dmn018.[1]
Li, S; Qayyum, A; Coakley, FV; Hricak, H (2000). "Association of renal agenesis and
mullerian duct anomalies.". Journal of computer assisted tomography. 24 (6):
829–34. PMID 11105695. doi:10.1097/00004728-200011000-00001.
Heinonen, PK (2006). "Complete septate uterus with longitudinal vaginal
septum.". FertilityandSterility. 85 (3):7005. PMID 16500341. doi:10.1016/j.fer
tnstert.2005.08.039.
British Woman With 2 Wombs Has Triplets. Associated Press, 22 December 2006.
http://www.uwmedicine.org/health-library/Pages/congenital-anomalies-of-the-
uterus.aspx](https://image.slidesharecdn.com/uterinemalformation-200912082625/75/Uterine-malformation-Define-Types-Diagnosis-Test-Treatment-in-word-File-Use-in-Clinical-submission-Of-OBG-9-2048.jpg)

This document discusses uterine malformations, which result from abnormal development of the Müllerian duct during embryogenesis. It describes the different classifications of uterine malformations according to the American Fertility Society. The most common type is a septate uterus, which occurs when the intervening uterovaginal septum fails to completely resorb after the Müllerian ducts fuse. Surgical resection of a uterine septum can help decrease miscarriage rates for women with this anomaly. The document also discusses the normal development of the female reproductive system from the Müllerian ducts and how failures during this process can lead to various uterine malformations.























































































