Downloaded 102 times
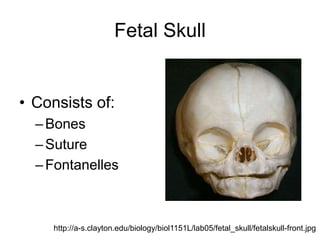
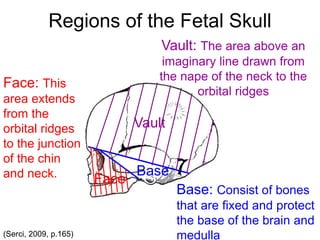
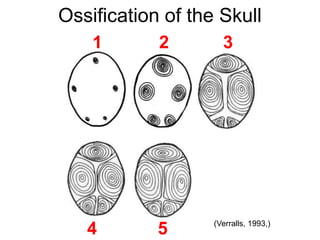
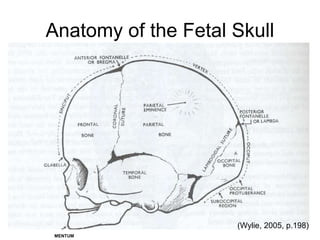
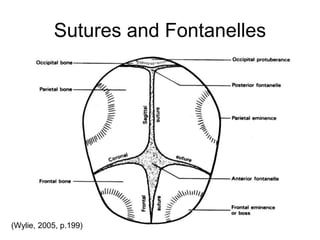
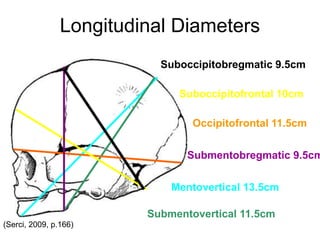
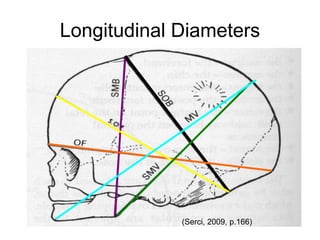
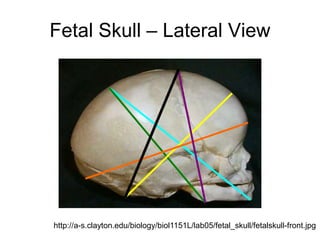
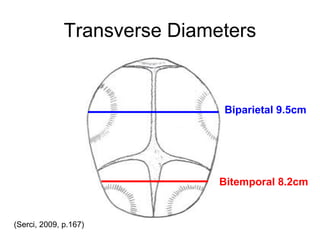
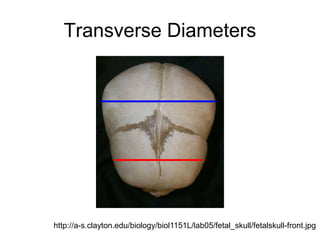
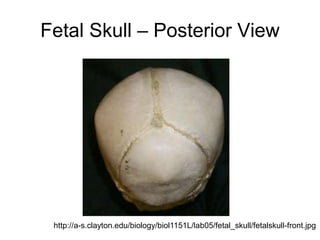
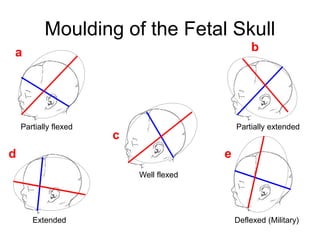
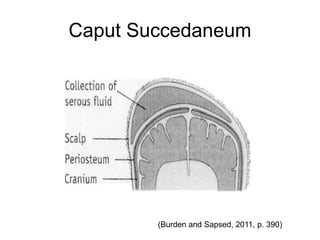
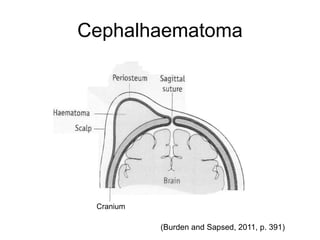
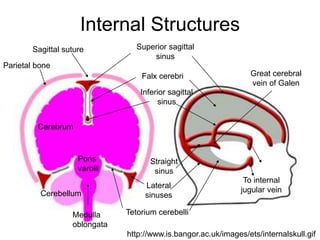

The document discusses the anatomy of the fetal skull. It describes the bones, sutures, fontanelles and regions of the skull. It outlines the ossification process and diameters used to measure the skull. Moulding is explained as the overlapping of skull bones during birth to decrease diameters. Potential injuries like caput succedaneum and cephalhematoma are also summarized.





















































































