2. Location and Description
a muscular tube about 10 in. (25 cm) long,
extending from the pharynx to the stomach
begins at the level of the cricoid cartilage,
opposite the body of the sixth cervical vertebra
It commences in the midline, but as it descends
through the neck, it inclines to the left side.
Passes through the diaphragm at the level of the
10th thoracic vertebra to join the stomach
3.
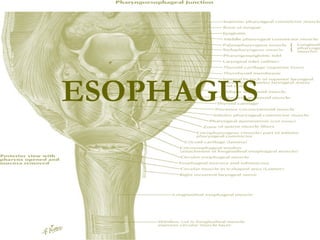
4. Musculature of Esophagus
The primary muscle of the upper
esophageal sphincter is the
cricopharyngeus portion of the inferior
pharyngeal constrictor.
The orientation of the muscles
Inner = Circular
Outer = Longitudinal
5.
6. Location and Description
Anteriorly
The trachea
the recurrent laryngeal nerves ascend one on
each side, in the groove between the trachea
and the esophagus
Posteriorly
The prevertebral layer of deep cervical fascia
the longus colli
the vertebral column
Laterally
On each side lie the lobe of the thyroid gland
and the carotid sheath
7.
8.
9. Blood Supply
Arterial Supply
1. upper third of the esophagus is supplied by the
inferior thyroid artery
1. middle third by branches from the descending
thoracic aorta
1. lower third by branches from the left gastric
artery
10.
11. Blood Supply
Venous drainage
1. veins from the upper third drain into the inferior
thyroid veins
1. middle third into the azygos veins
1. the lower third into the left gastric vein, a
tributary of the portal vein
12.
13. Lymph drainage
1. upper third of the esophagus drain into the deep
cervical nodes
1. middle third into the superior and posterior
mediastinal nodes
1. lower third into nodes along the left gastric
blood vessels and the celiac nodes
14.
15. Nerve Supply
The nerves are derived from the recurrent
laryngeal nerves and from the sympathetic
trunks
In the lower part of its thoracic course, the
esophagus is surrounded by the
esophageal nerve plexus.
16.
17. Clinical Notes
Esophageal Constrictions
The esophagus has three anatomic and physiologic
constrictions. The first is where the pharynx joins the upper
end, the second is where the aortic arch and the left bronchus
cross its anterior surface, and the third occurs where the
esophagus passes through the diaphragm into the stomach.
These constrictions are of considerable clinical importance
because they are sites where swallowed foreign bodies can
lodge or through which it may be difficult to pass an
esophagoscope. Because a slight delay in the passage of food
or fluid occurs at these levels, strictures develop here after the
drinking of caustic fluids. Those constrictions are also the
common sites of carcinoma of the esophagus. It is useful to
remember that their respective distances from the upper
incisor teeth are 6 in. (15 cm), 10 in. (25 cm), and 16 in. (41
cm), respectively.
18.
19. Clinical Notes
Achalasia or Cardiospasm
The cause is unknown. The primary site of the
disorder maybe in the innervations of the
cardioesophageal sphincter by the vagus
nerve. Dysphagia (difficulty in swallowing) and
regurgitation are common symptoms.
Achalasia can be treated by surgically dilating
(enlarging) the esophagus.
20. Clinical Notes
Gastroesophageal reflux disease (GERD)
is defined as the movement of gastric contents into the
esophagus without vomiting. GERD occurs when gastric
contents irritate mucosal surfaces of the upper aerodigestive
tract. It is the most common esophageal disease. Besides the
typical presentation of heartburn and acid regurgitation, either
alone or in combination, GERD can cause atypical symptoms.
An estimated 20 to 60 percent of patients with GERD have
head and neck symptoms without any appreciable heartburn.
While the most common head and neck symptom is a globus
sensation (a lump in the throat), the head and neck
manifestations can be diverse and may be misleading in the
initial work-up. Thus, a high index of suspicion is required.
22. Clinical Notes
Esophageal
atresia
is a congenital
medical condition
which affects the
alimentary tract.
It causes the
esophagus to end
in a blind-ended
pouch rather than
connecting
normally to the
stomach.
23. Clinical Notes
Esophagitis
Inflammation of the esophagus
Causes include
infection such as candida and herpes
simplex
chemical injury by alkaline and acid
solutions
fungi