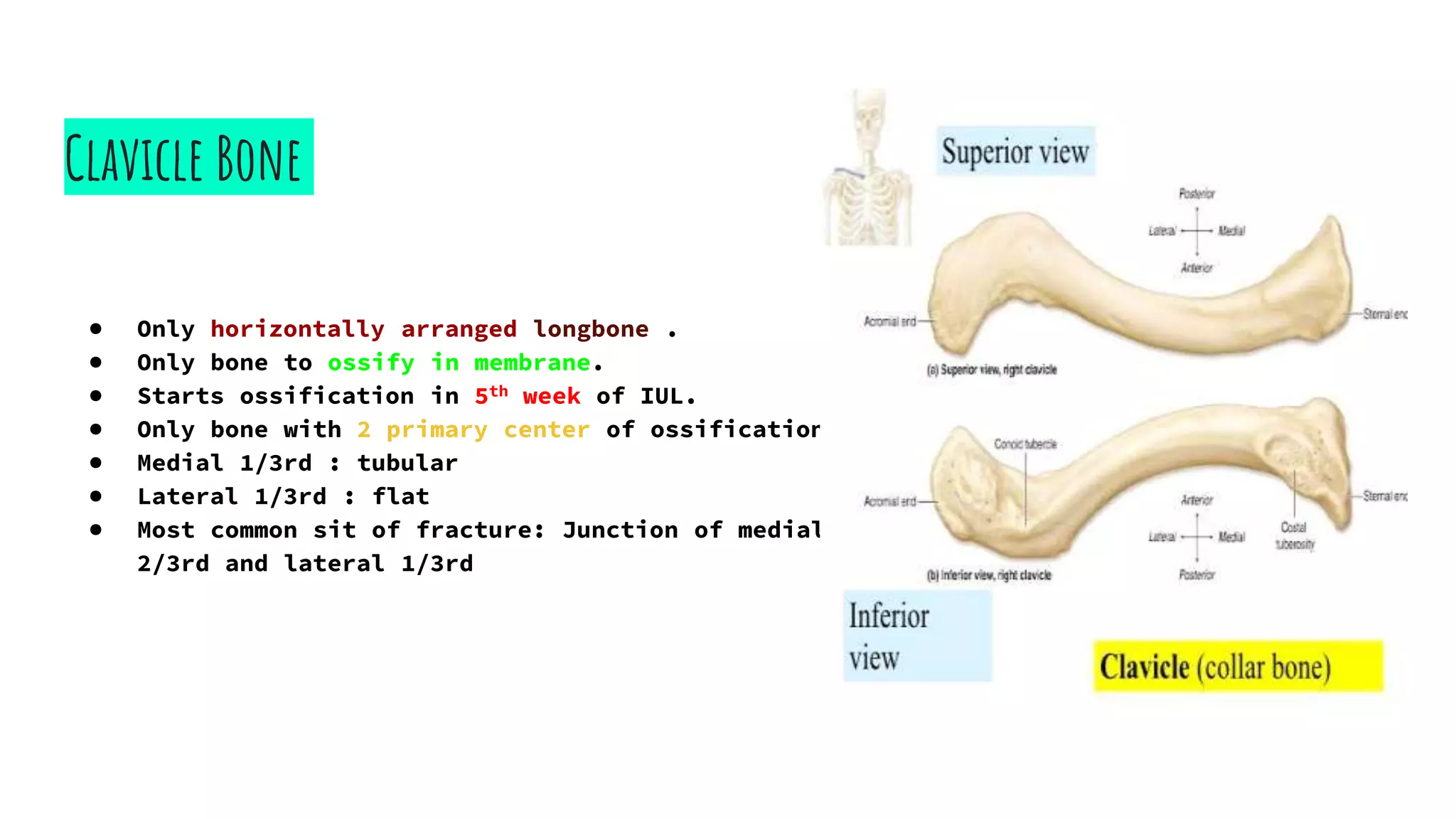
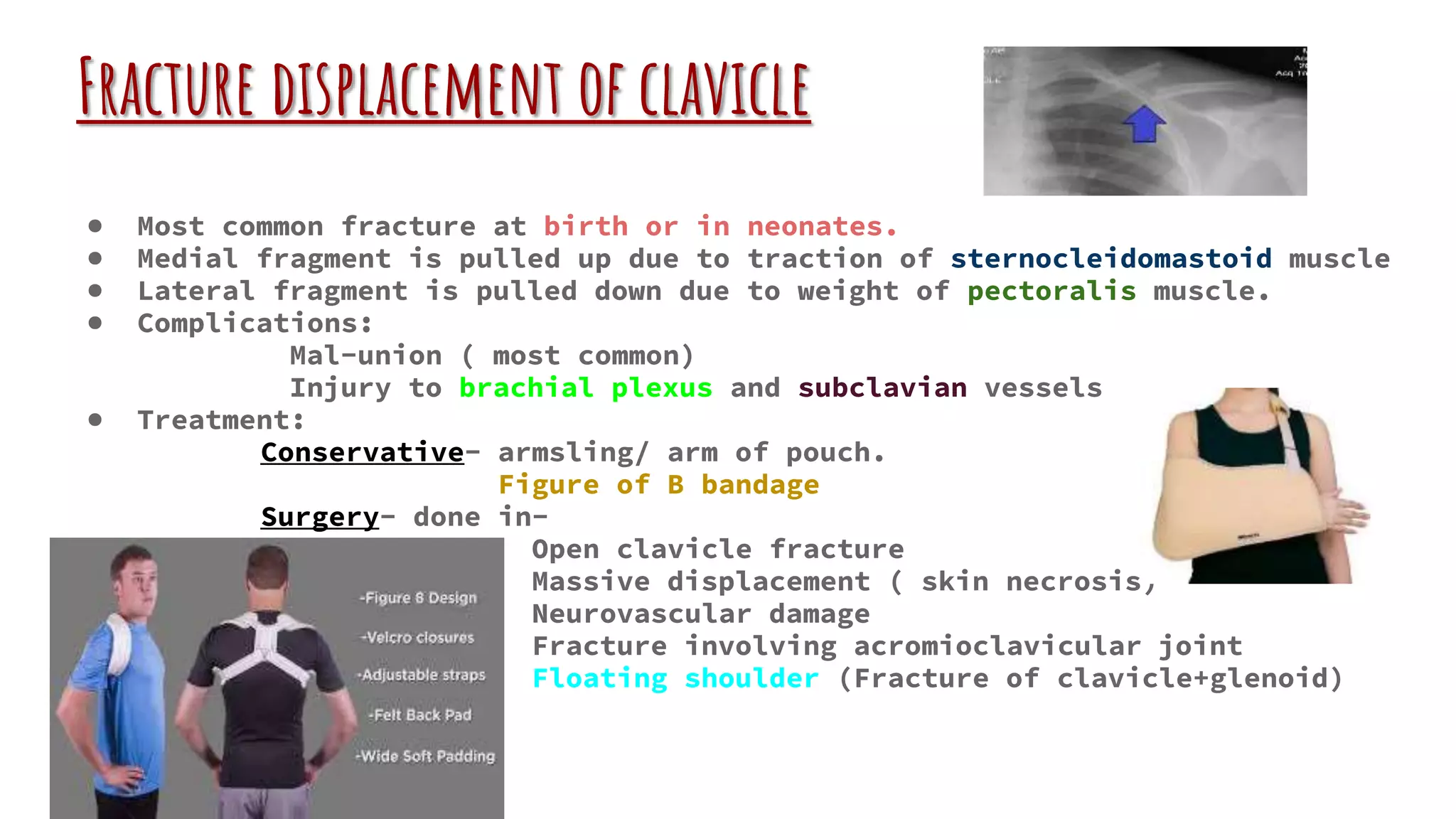
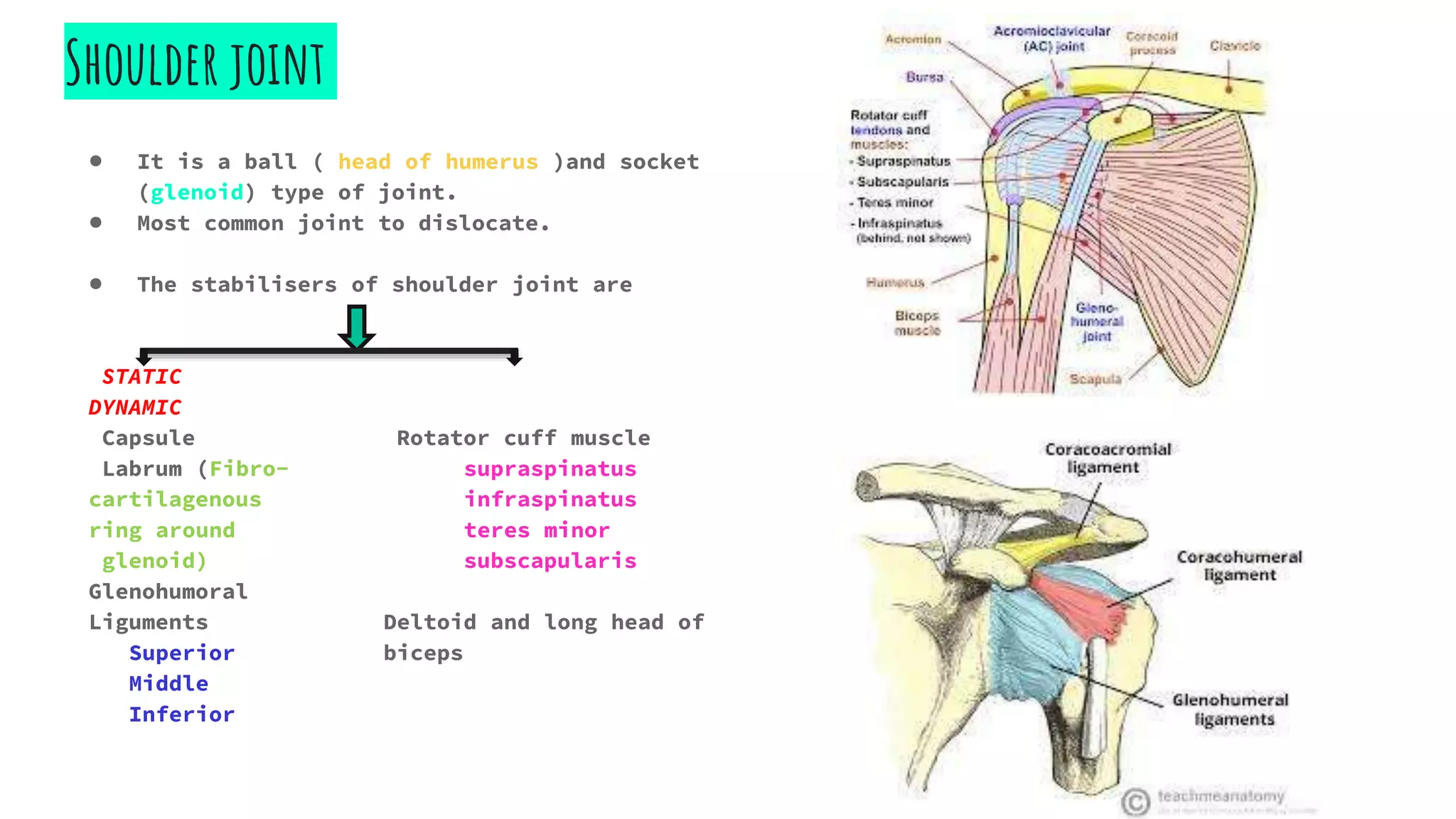
The document discusses upper limb fractures, specifically focusing on clavicle and shoulder joint injuries. It details characteristics of the clavicle, common fracture types, treatment methods, and complications of shoulder dislocation, including tests for diagnosis and management strategies. Additionally, it covers various lesions associated with recurrent dislocations and outlines surgical procedures for shoulder instability.