The document discusses injuries around the shoulder joint, including:
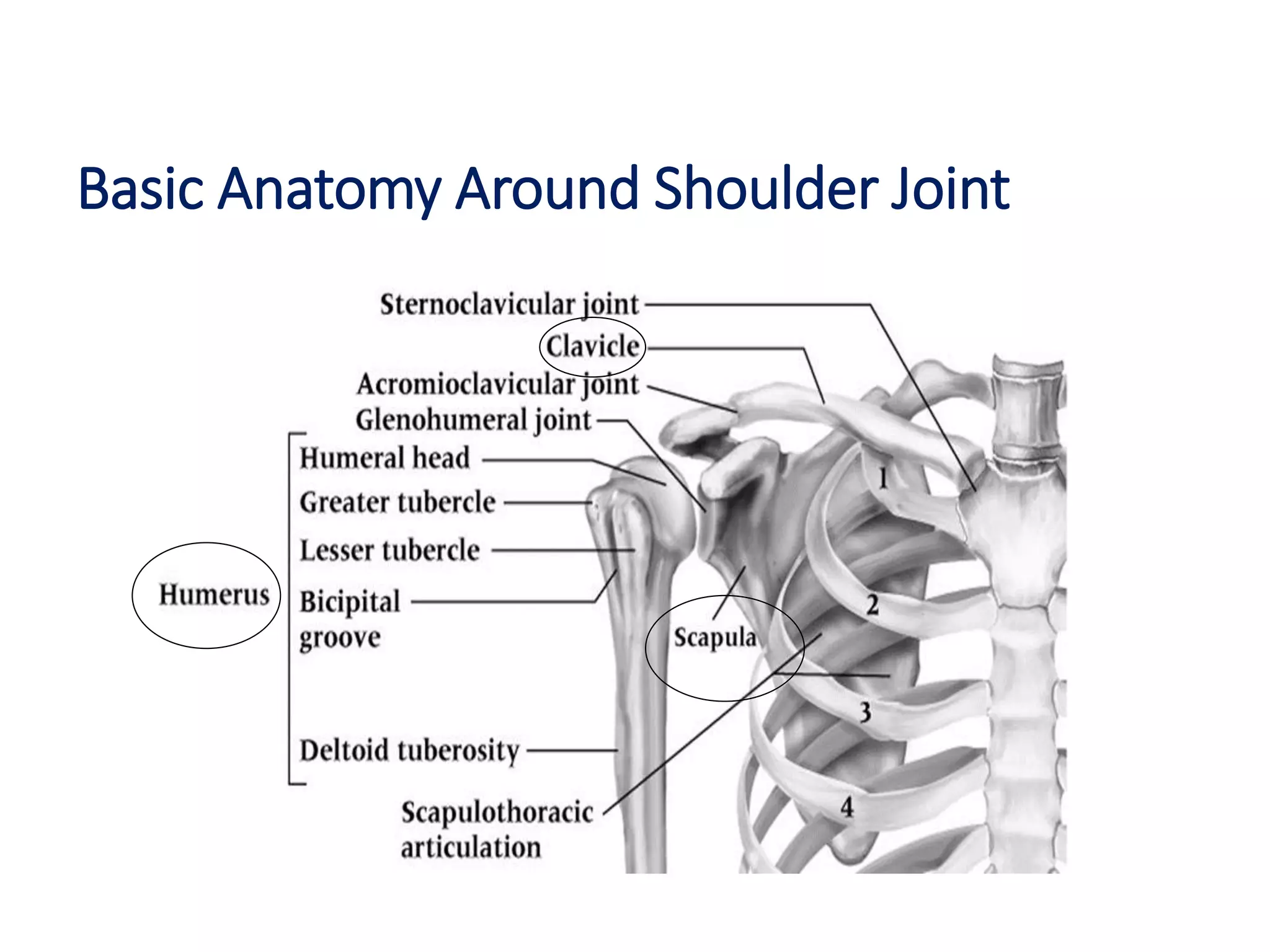
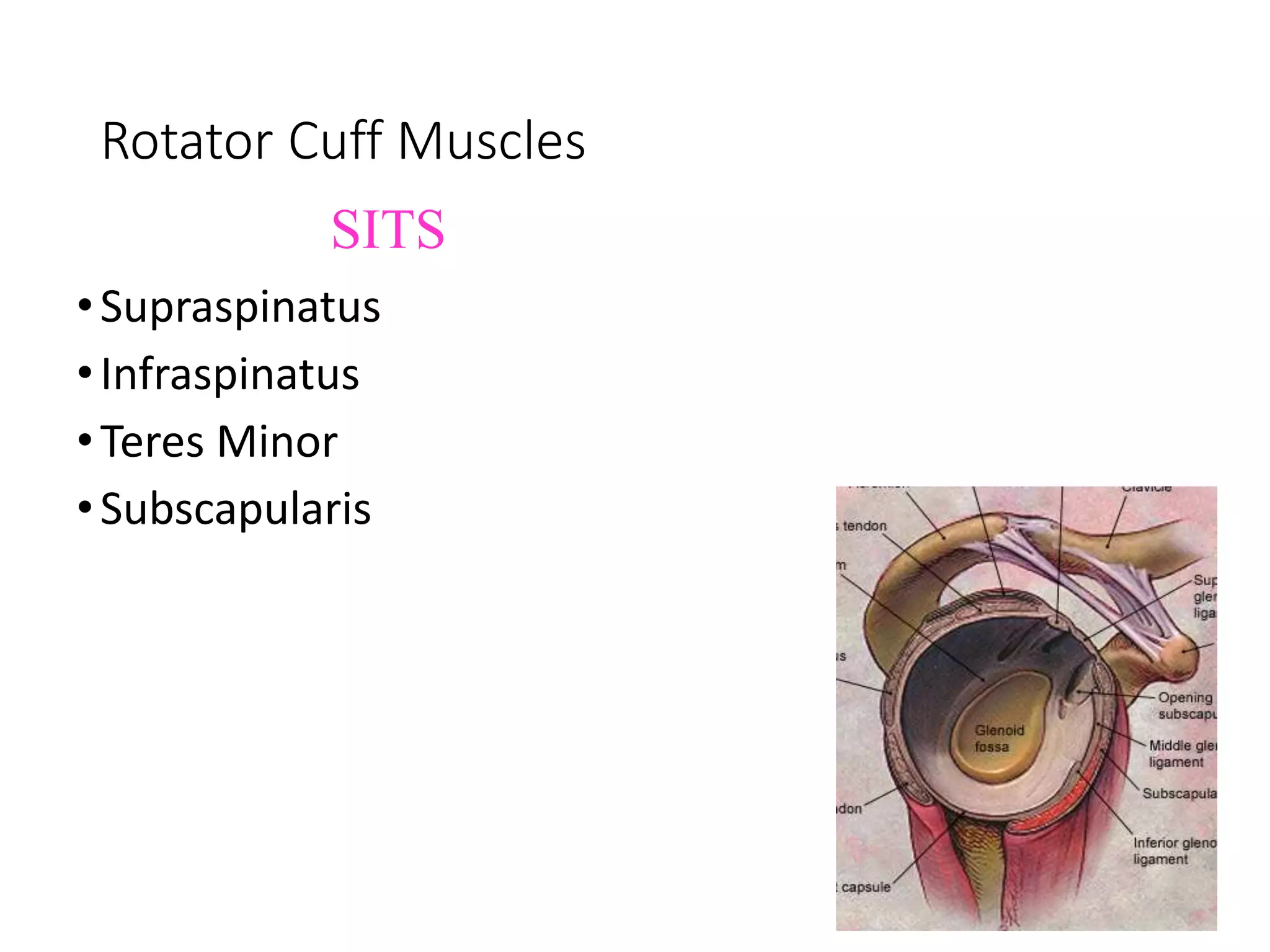
- Basic anatomy of the shoulder joint and its stabilizing muscles and ligaments.
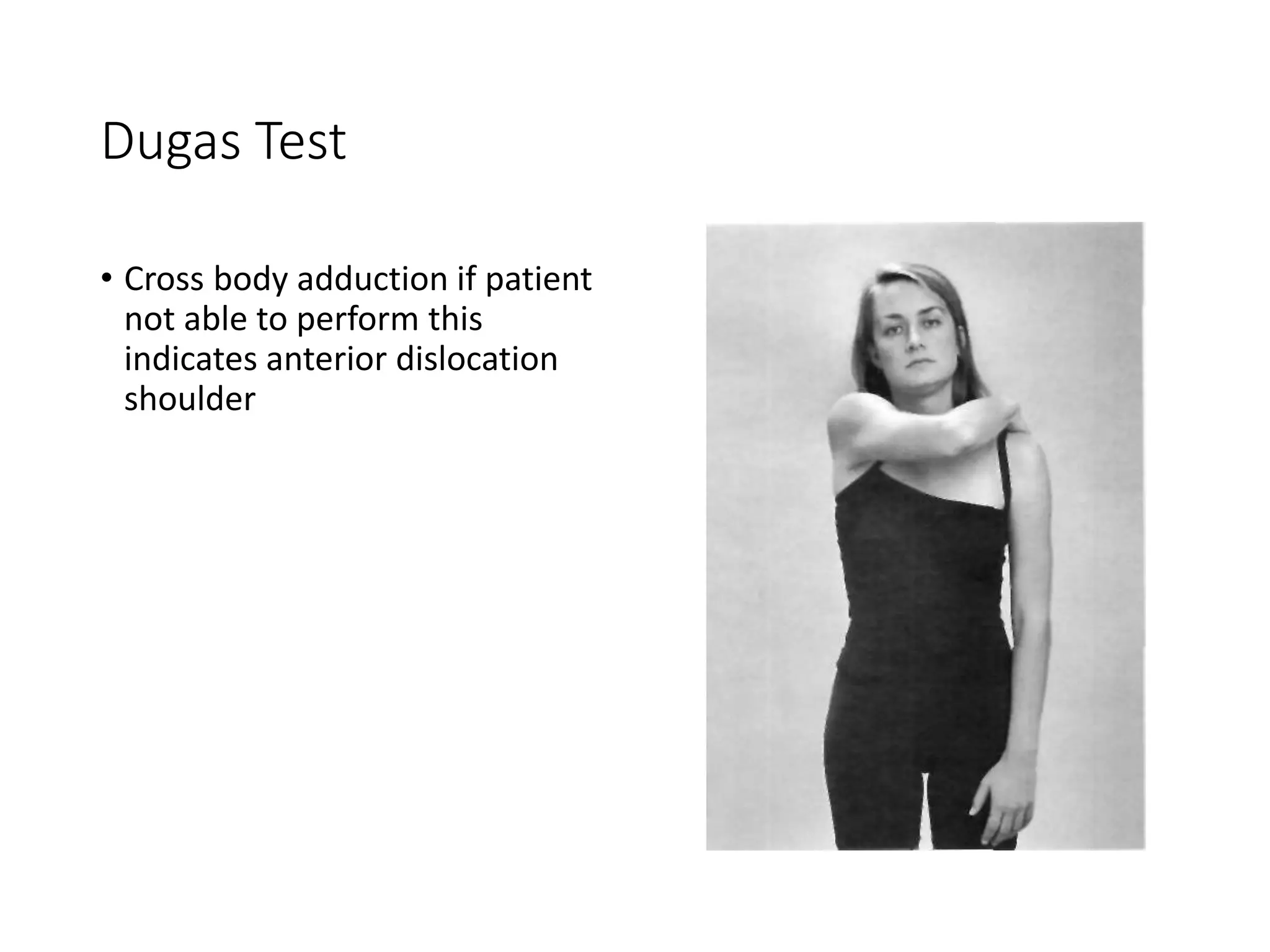
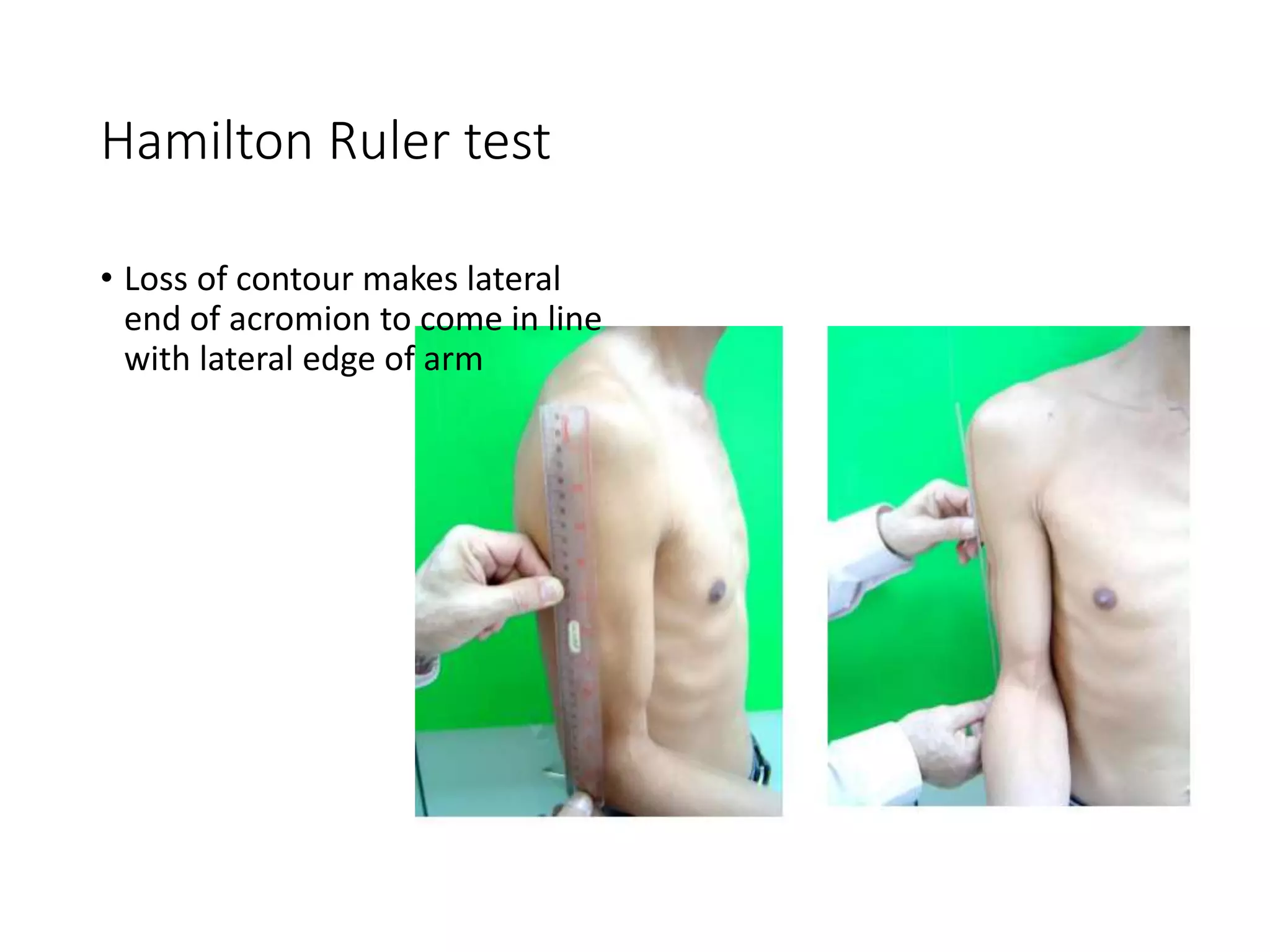
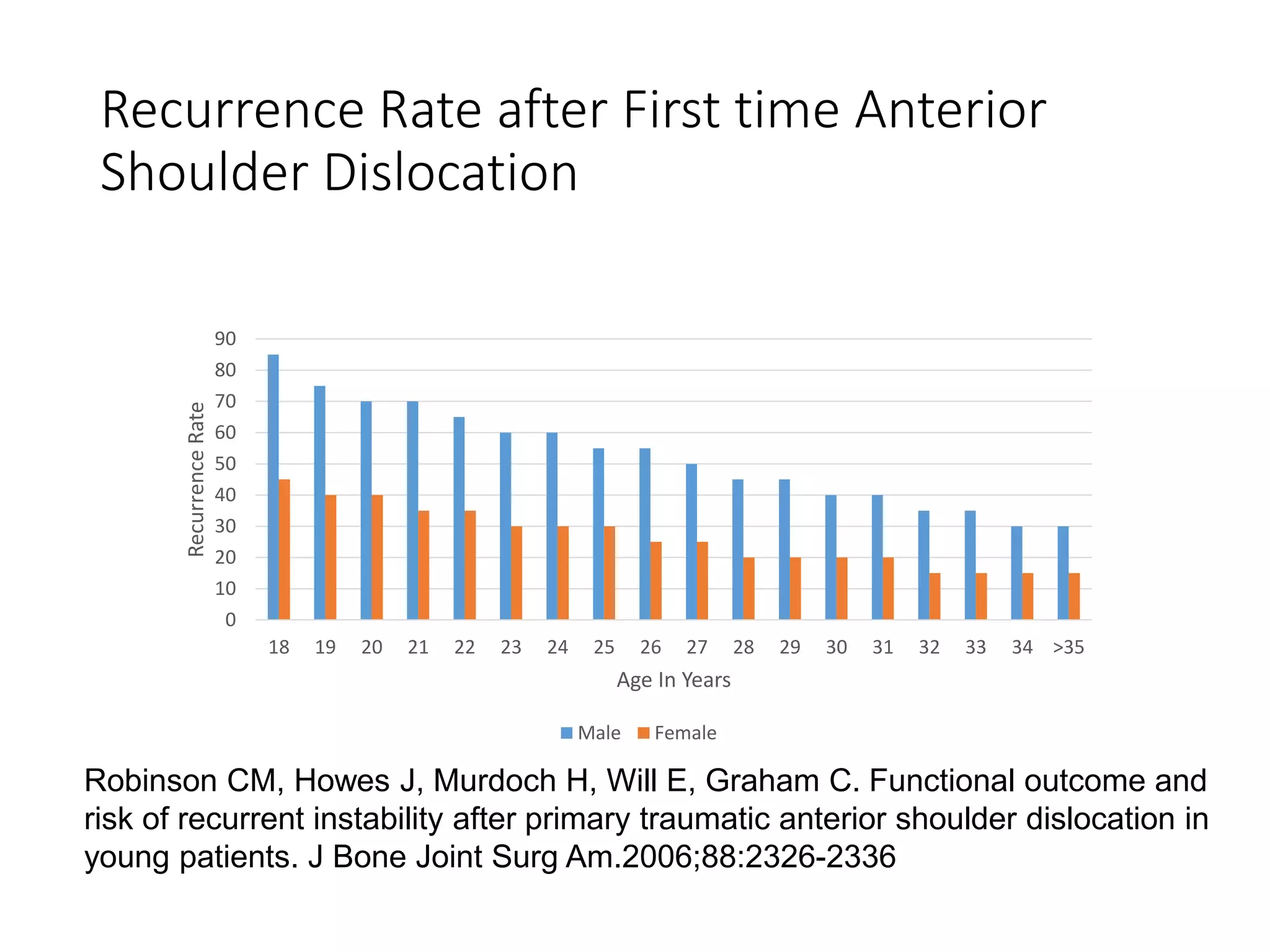
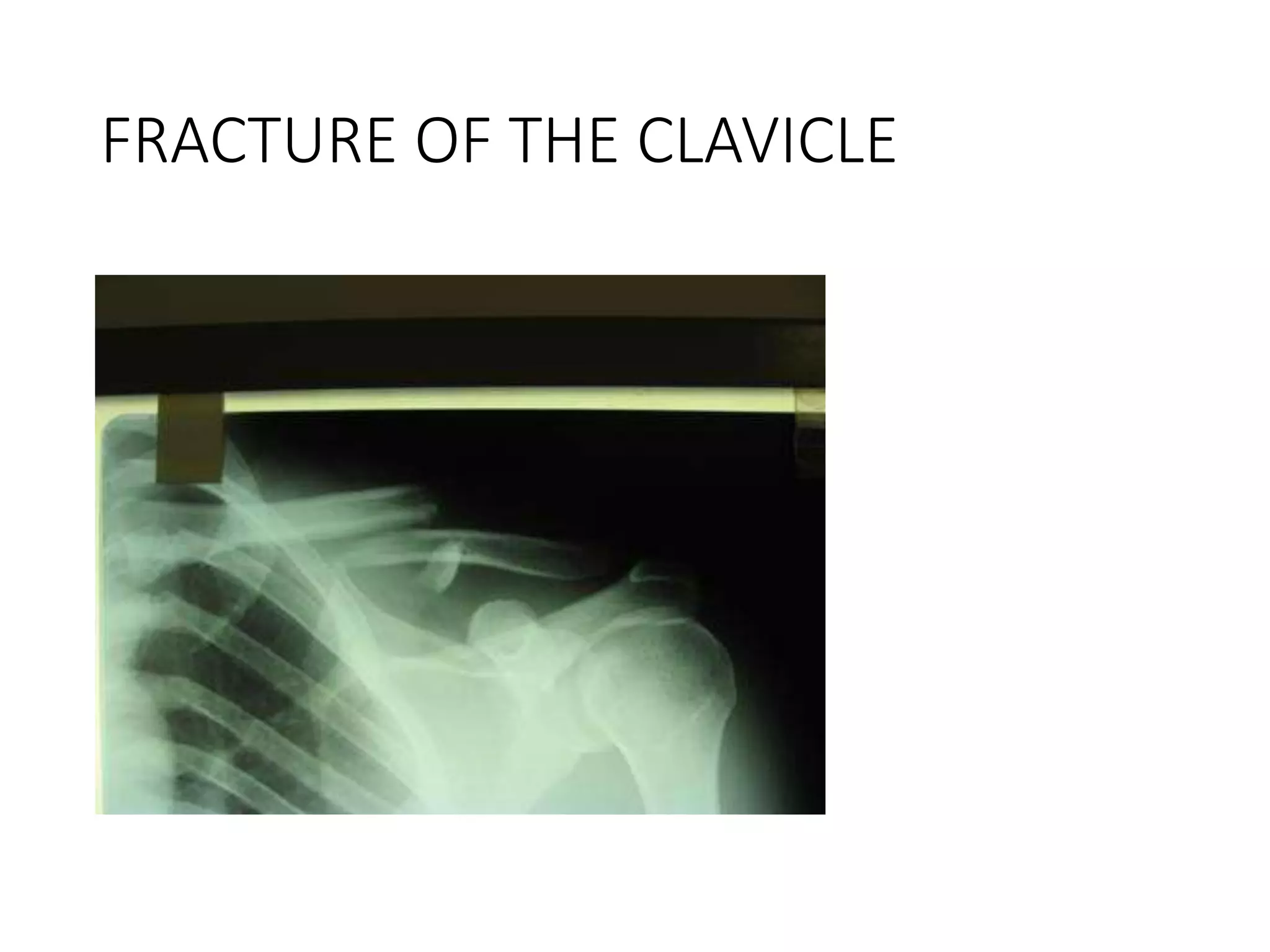
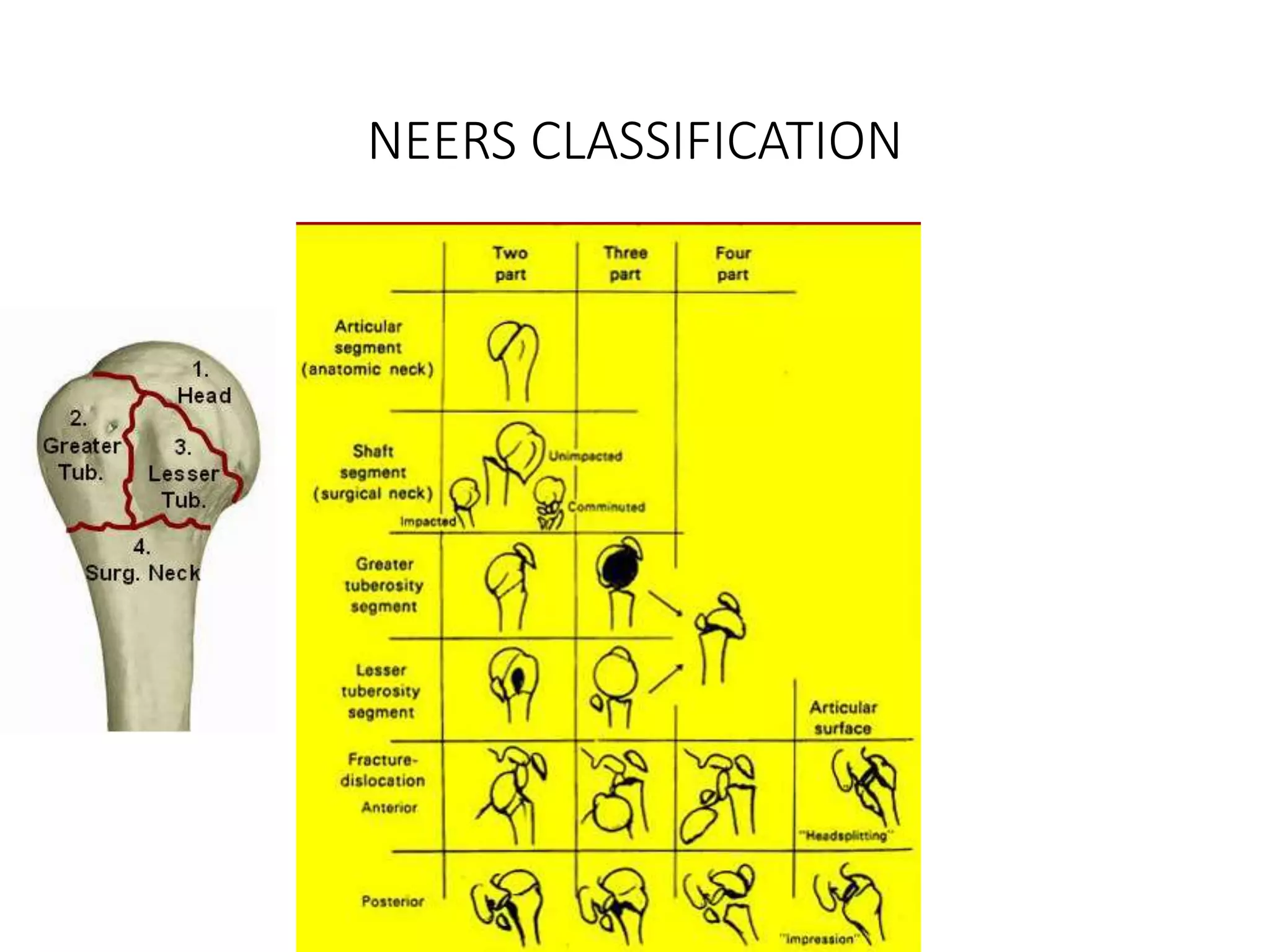
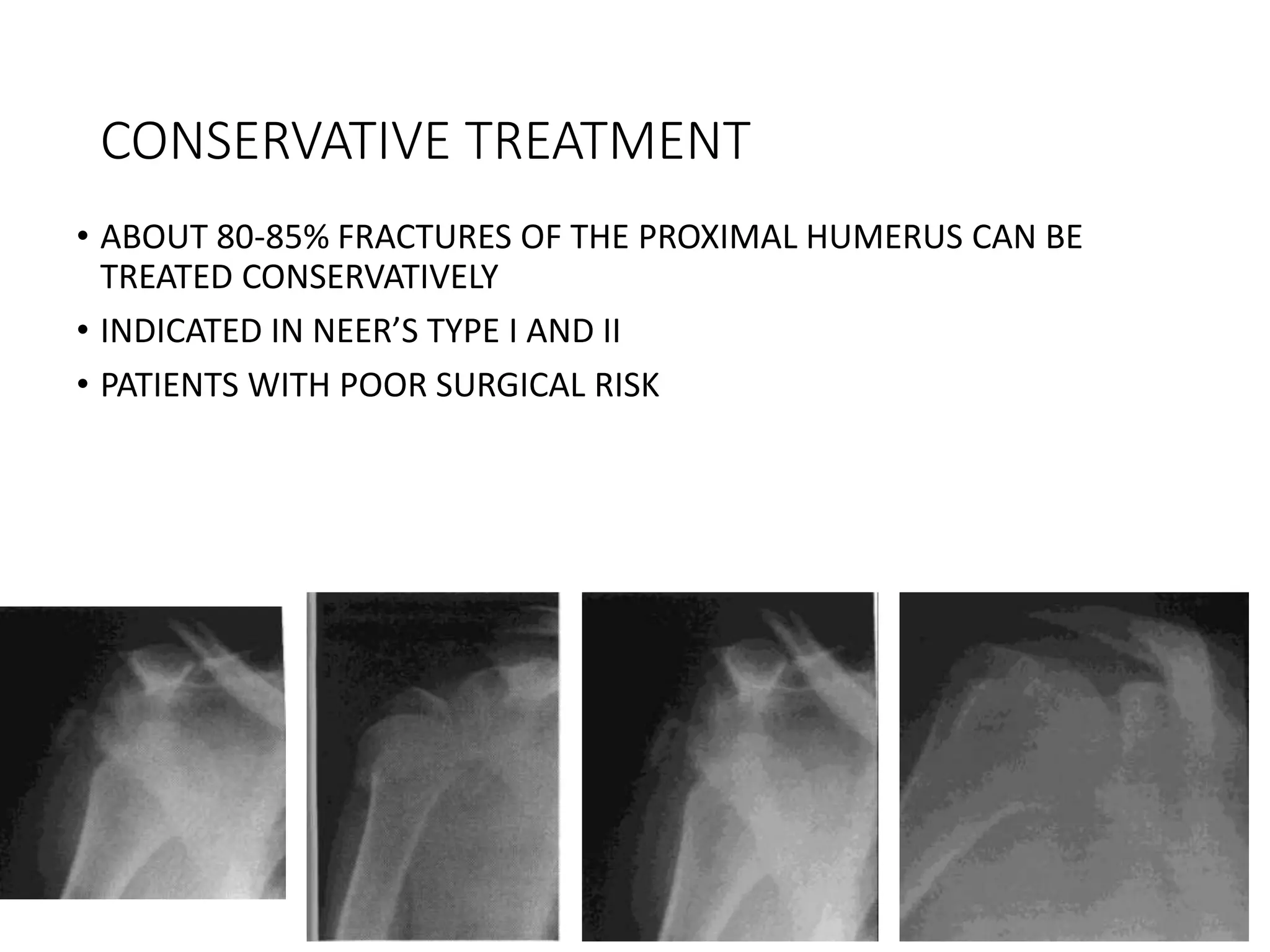
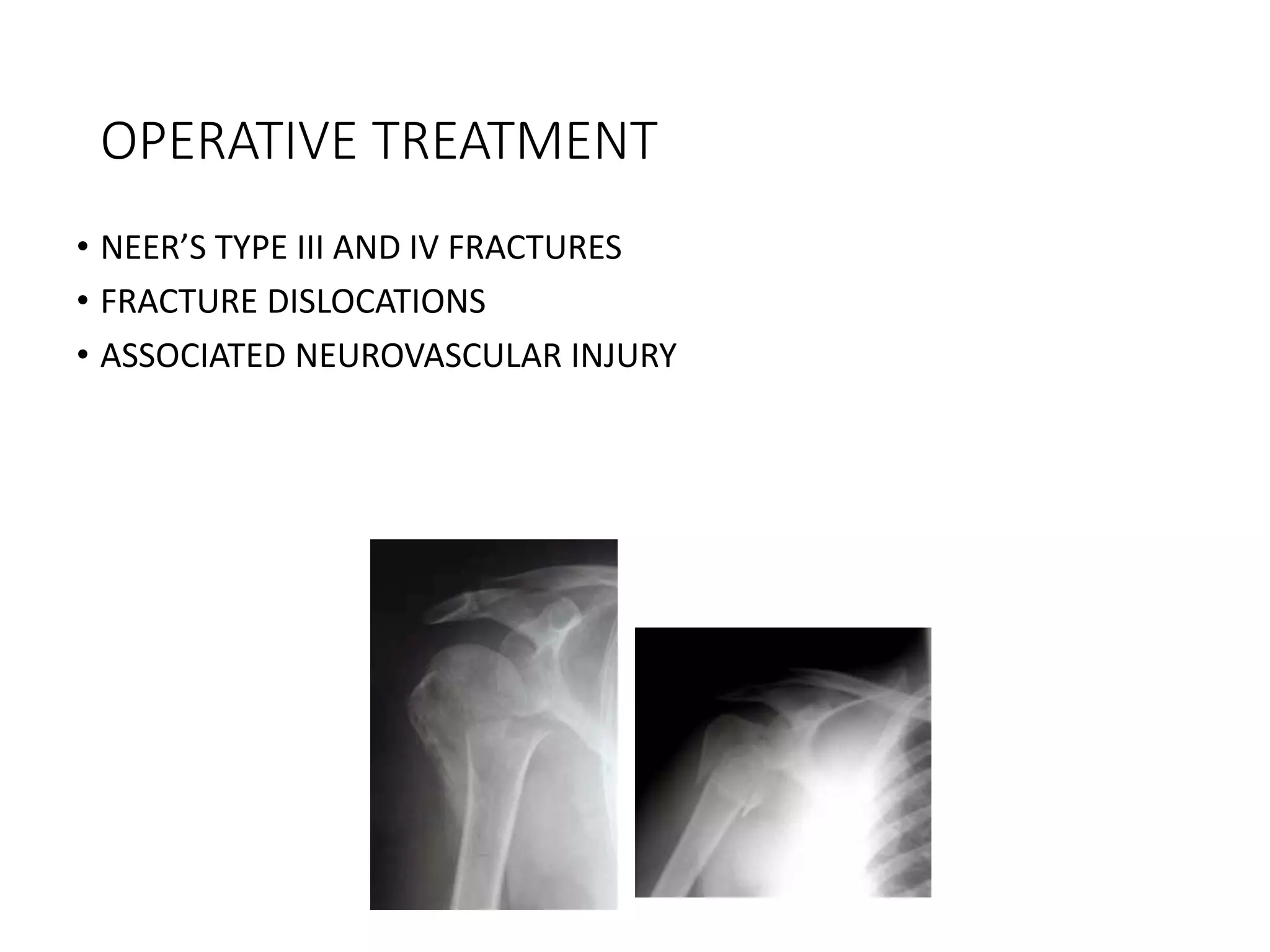
- Common injuries like anterior dislocation, fractures of the clavicle and proximal humerus.
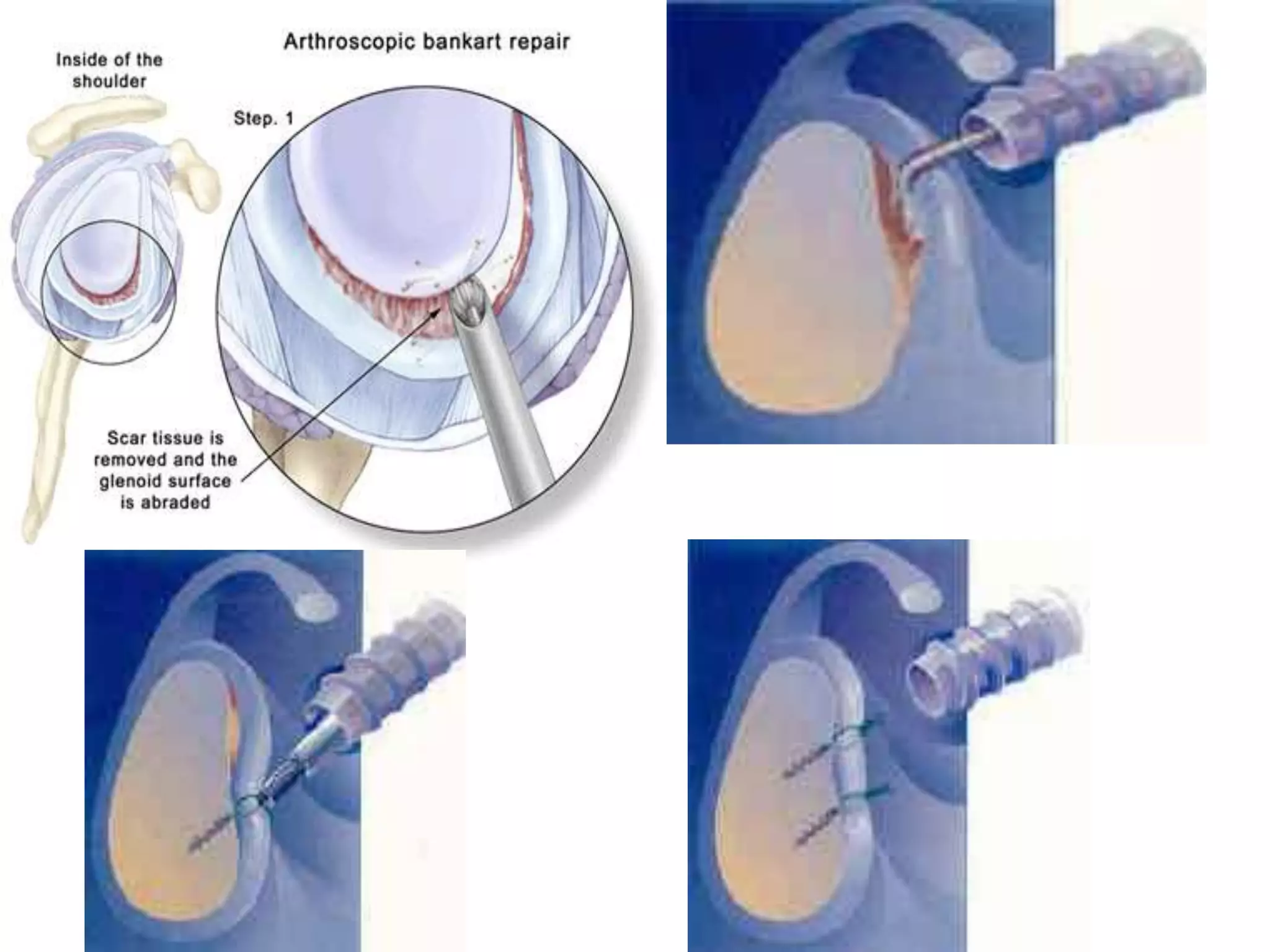
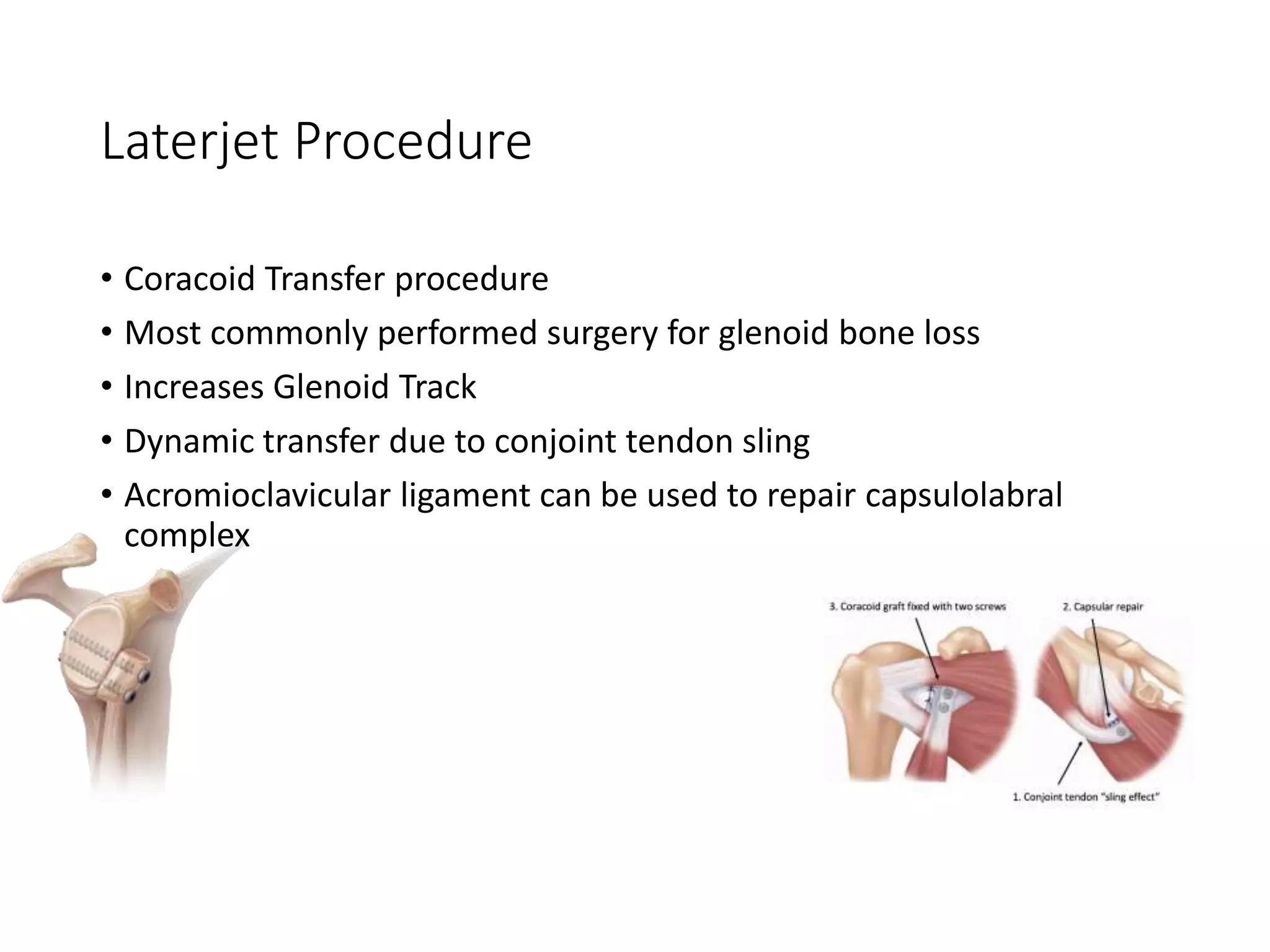
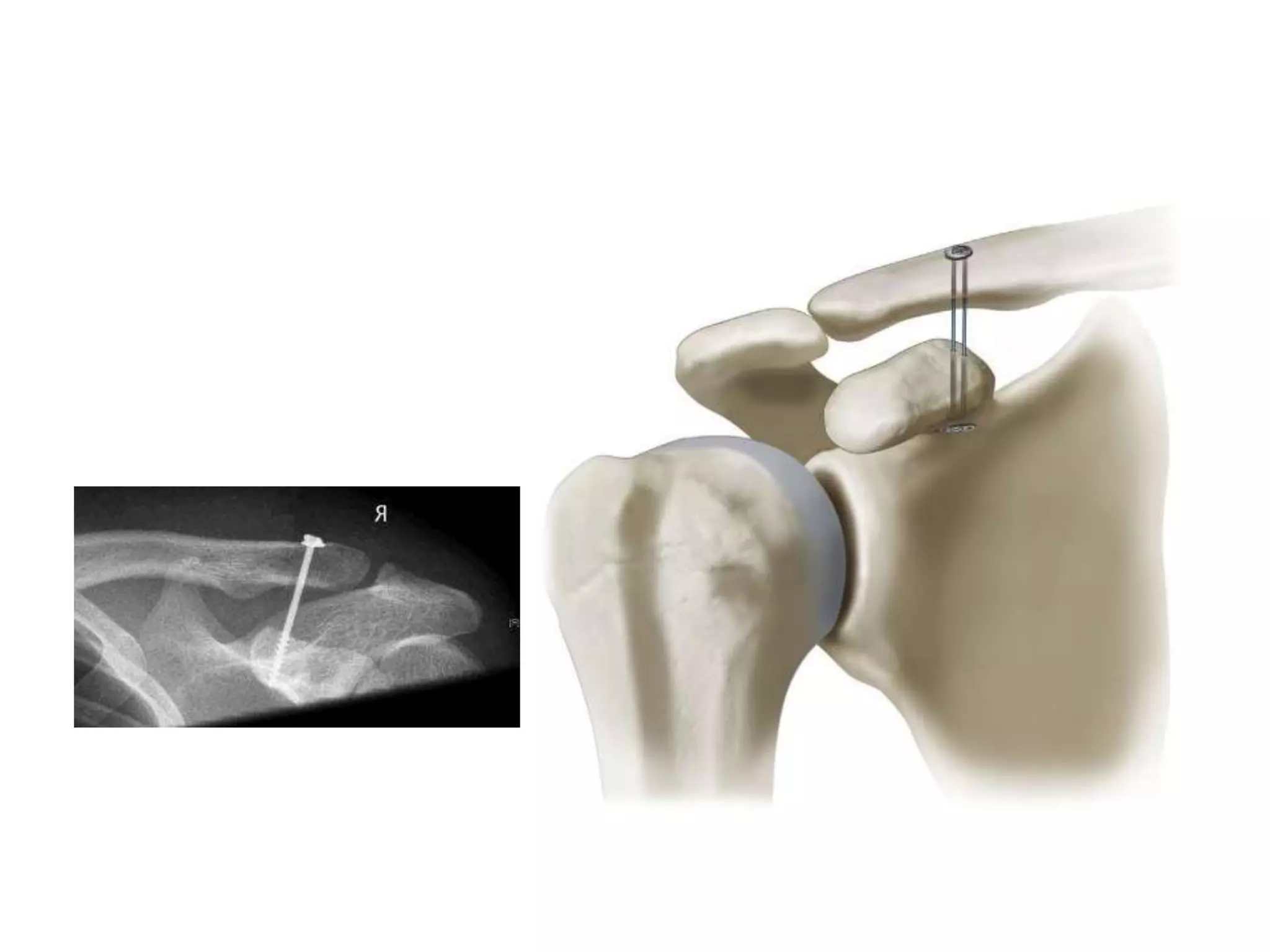
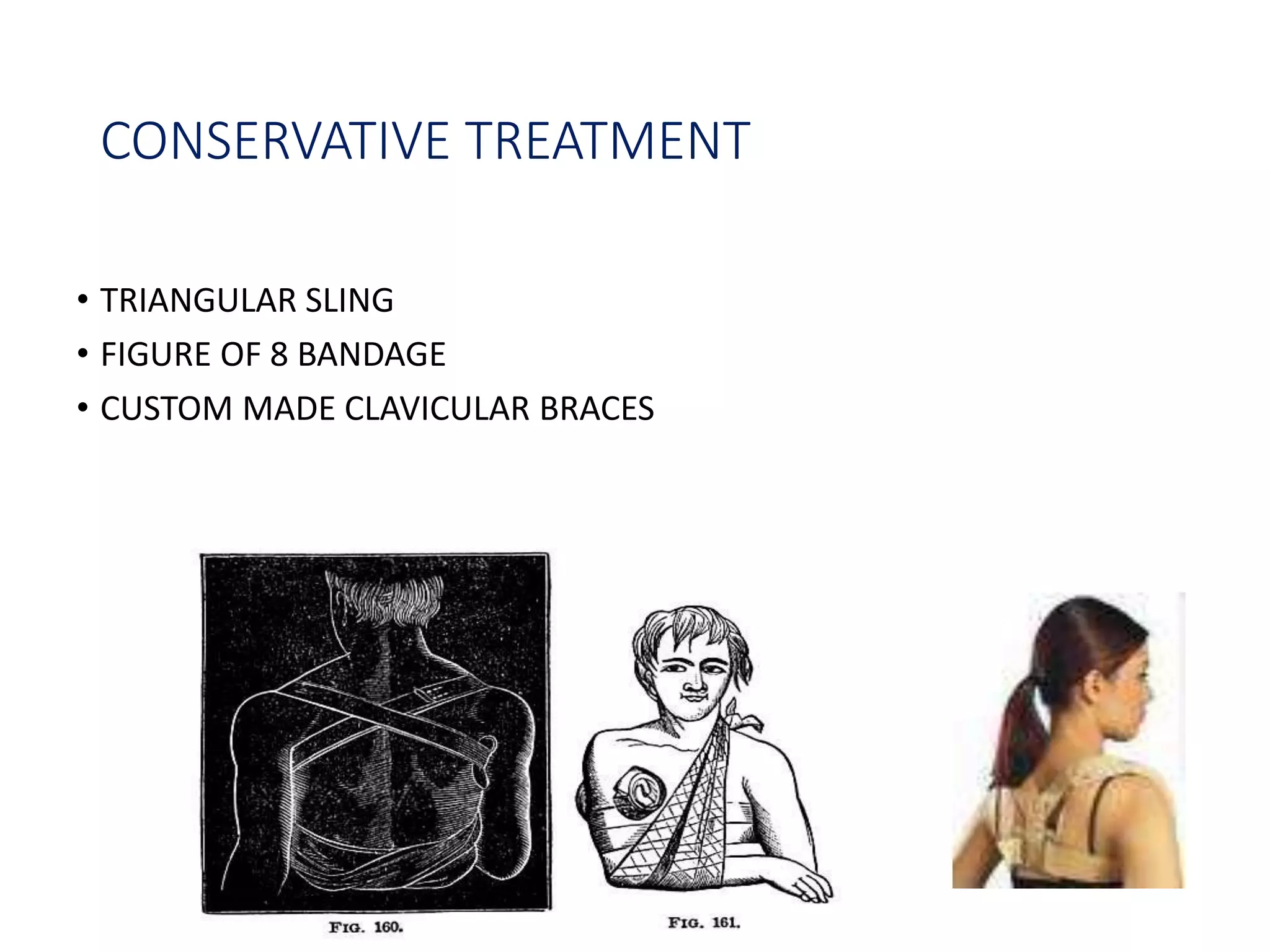
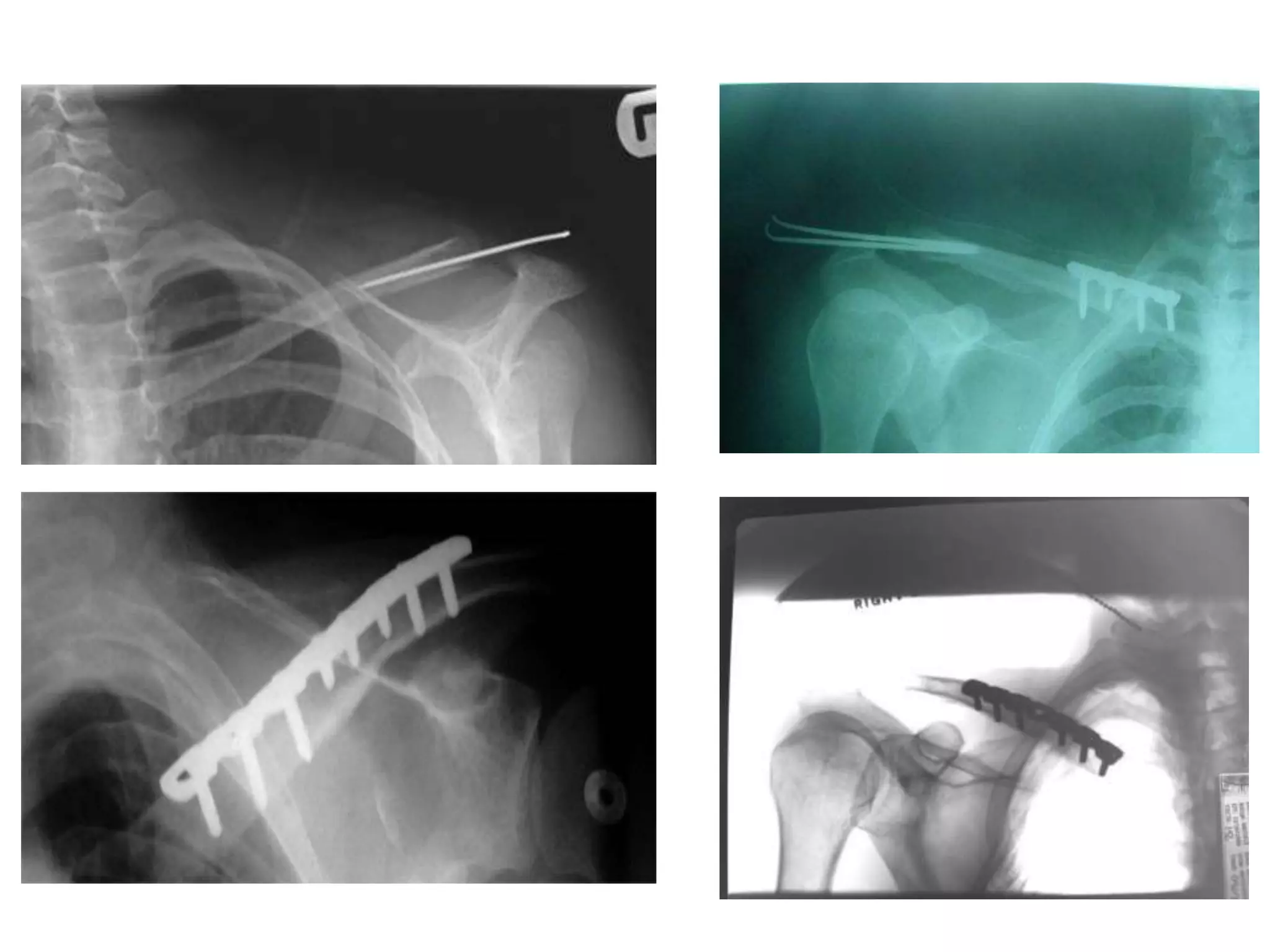
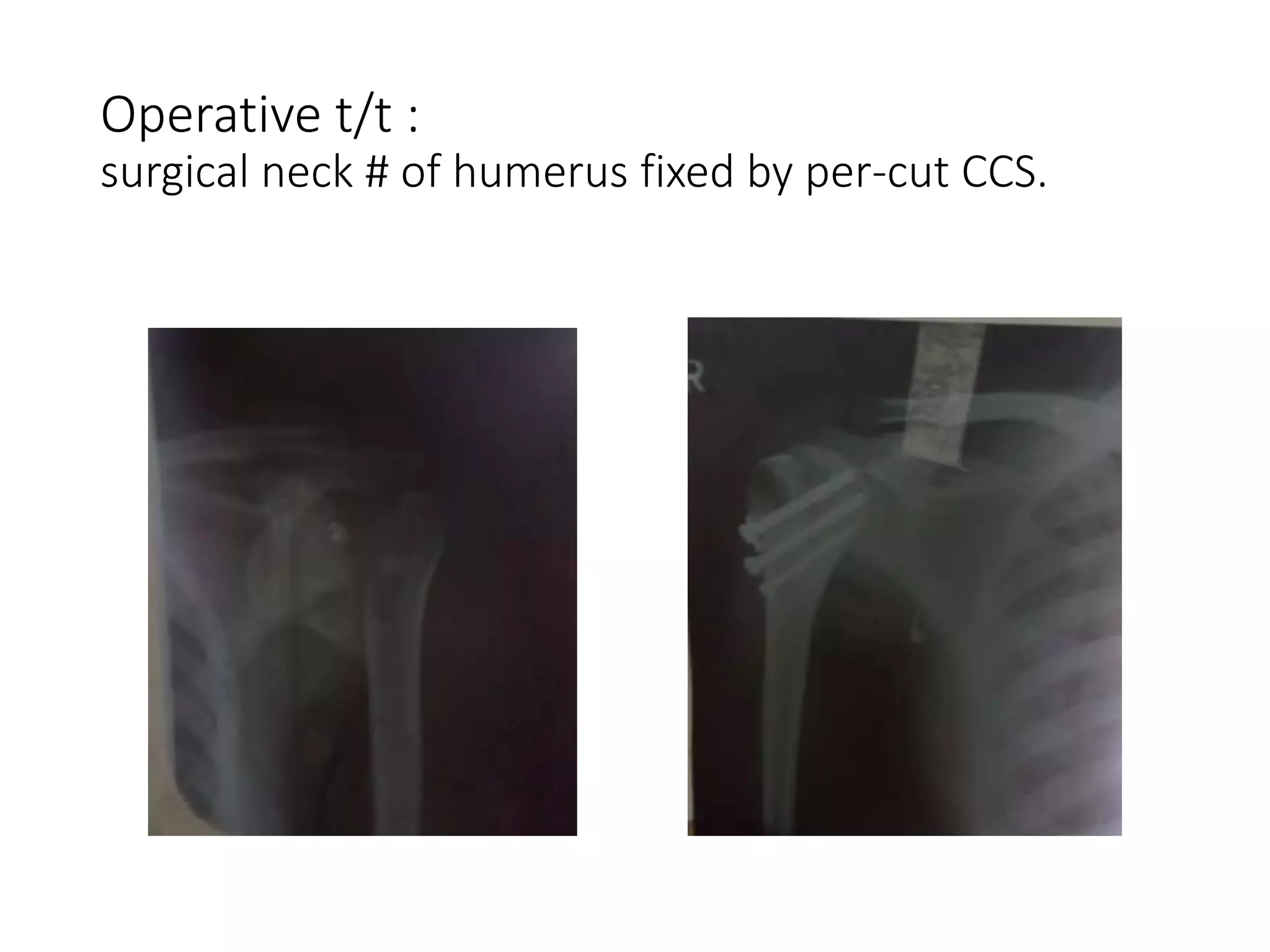
- Treatment approaches for these injuries including closed/open reduction, immobilization, and surgical repair or reconstruction depending on the injury type and chronicity.