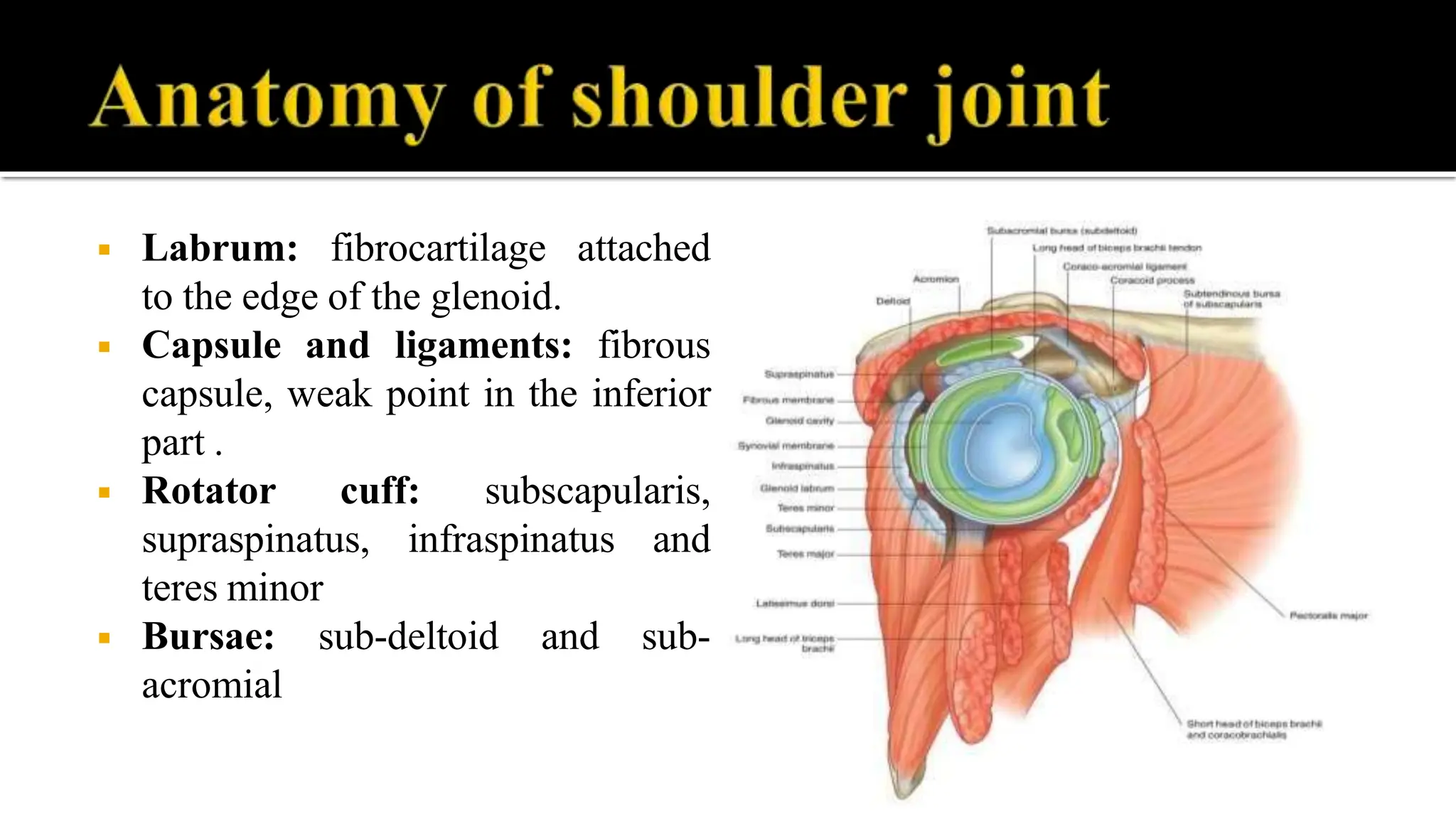
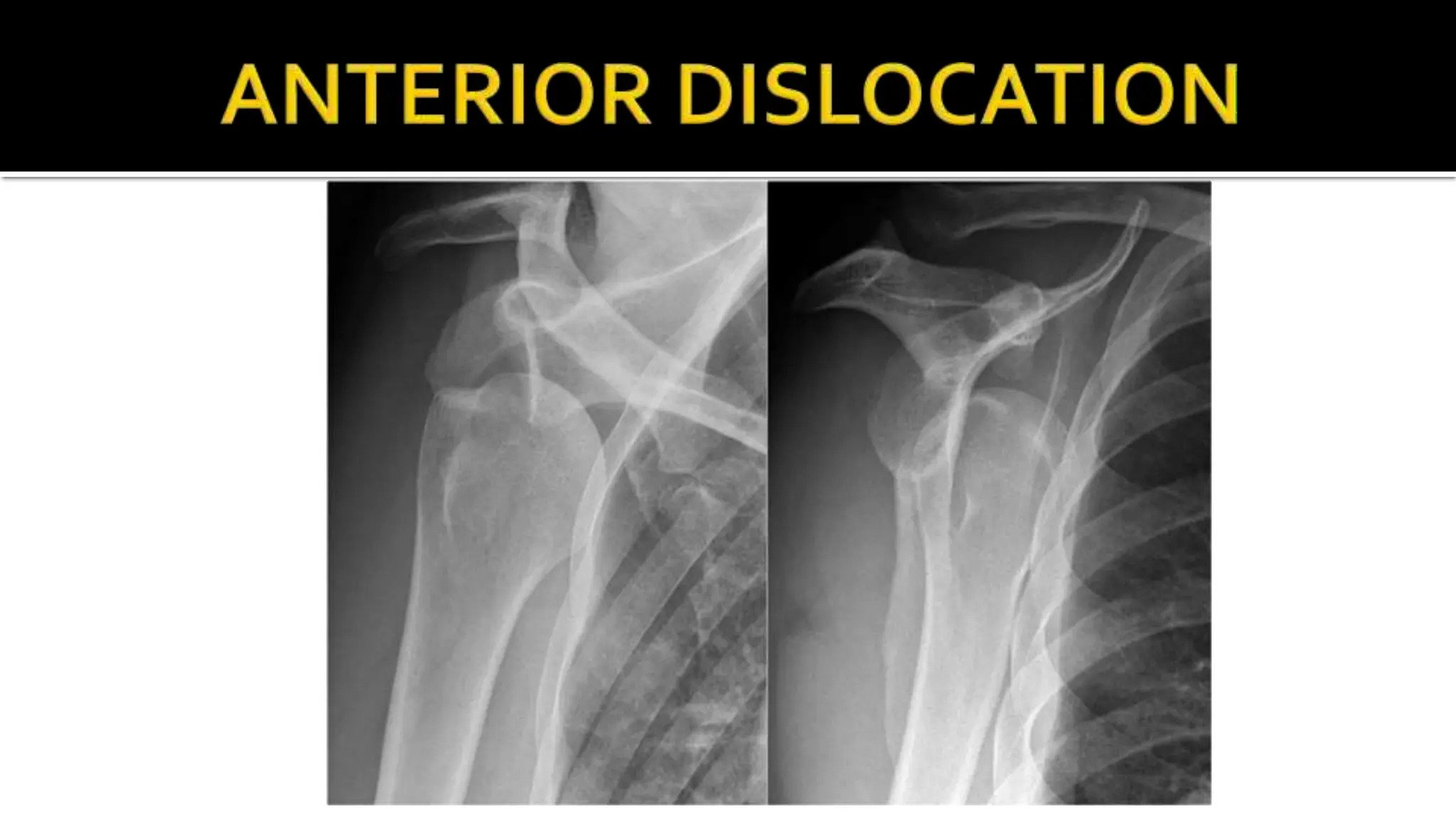
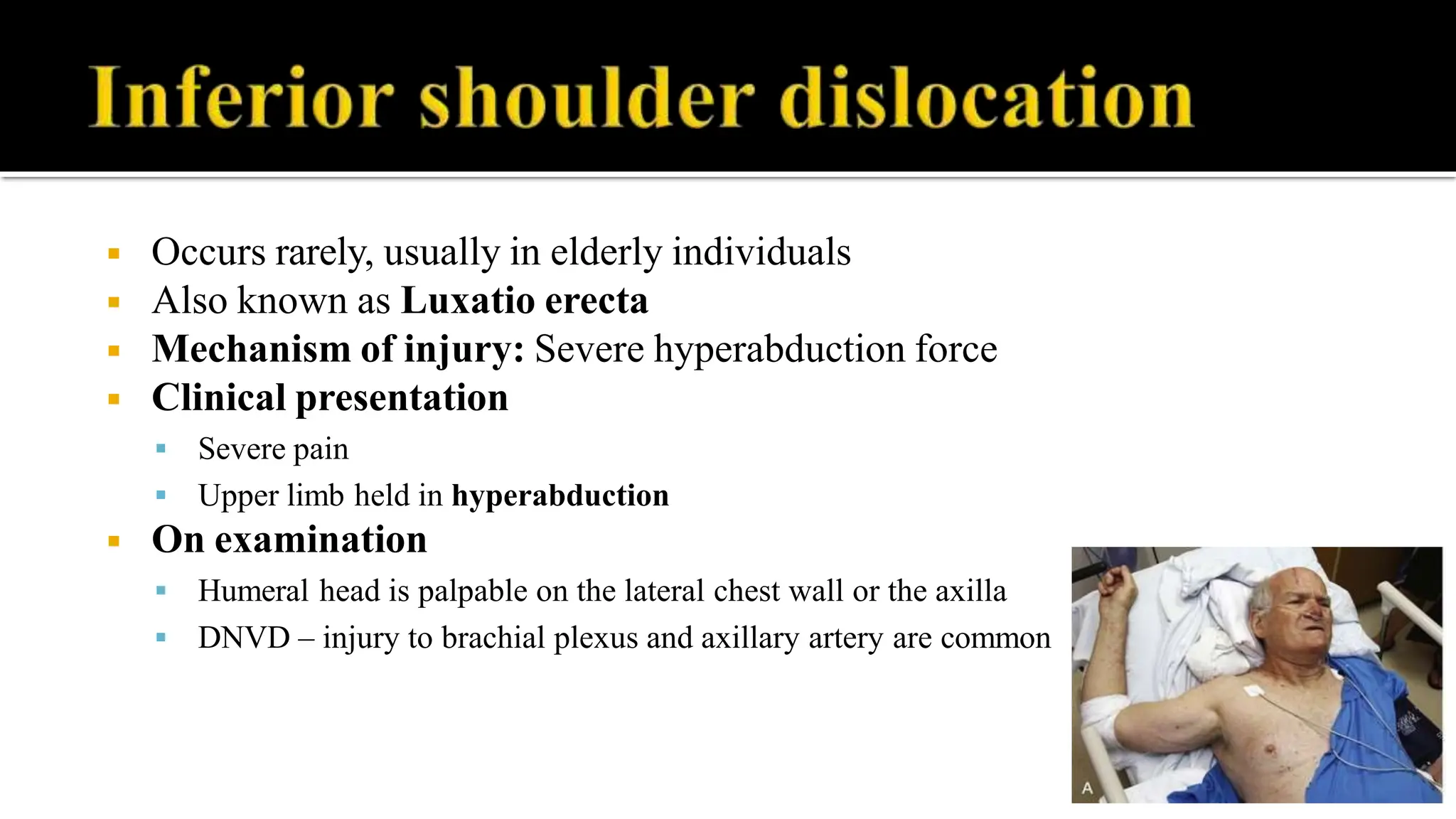
The document discusses the anatomy, mechanisms, clinical presentation, and treatment of shoulder dislocations, including both anterior and posterior dislocations as well as the rare luxatio erecta. It covers complications, diagnostic methods such as X-rays and MRI, and treatment options like closed reduction techniques and surgical intervention. The text also elaborates on various pathological lesions associated with dislocations and the importance of physiotherapy post-reduction.