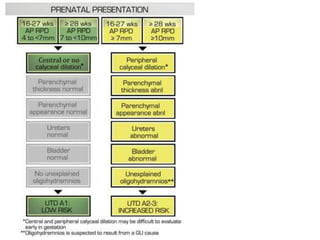
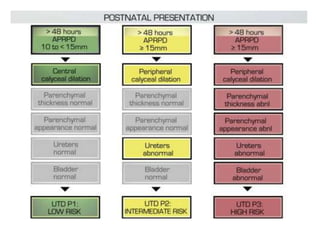
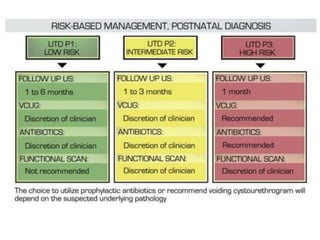
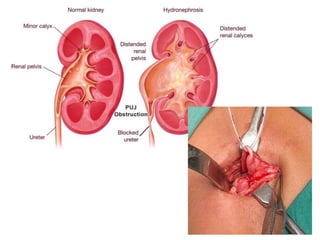
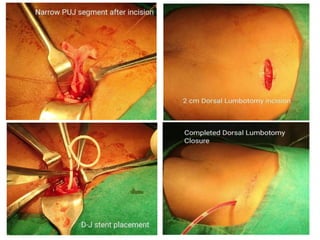
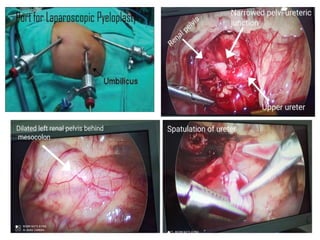
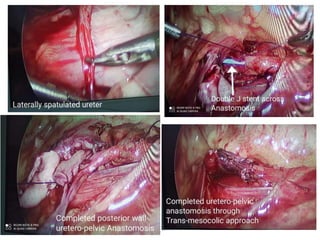
The document discusses pelvi-ureteric junction obstruction (PUJO), detailing causes, clinical presentations, diagnostics, and treatment options such as pyeloplasty. It highlights the importance of timely evaluation and various imaging techniques for accurate diagnosis and follow-up. Surgical techniques, including different types of pyeloplasty, are explored along with their associated complications and management in special circumstances.