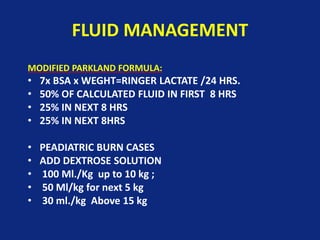
This document discusses electrical burn management. It notes that electrical burns are devastating injuries that often affect young, healthy males. They can cause damage beyond just the skin, including muscle contractions, internal organ damage, and complications like compartment syndrome. Management involves fluid resuscitation, wound care, investigations for internal injuries, and early surgery for debridement, fasciotomies, or amputations if needed. While challenging, efforts should be made to salvage limbs when possible through reconstructive surgeries and skin grafts. With timely treatment electrical burn survival has improved but morbidity remains high due to complications and functional limitations.