INTRODUCTION
• It isa serious life threatening injuries in children.
• It is due to thermal injury produced as an electrical current pass
through body.
• Amount of thermal injury produced is directly proportional to degree
of electric current.
• Children of age <6 yr are mostly injured due to low voltage outlet .
• Older children have an increased chance of injury by high voltage
current due to higher mobility and adventurousness.
3.
IMPORTANCE
• It isa burn injury but it is dangerous because it leads to cardiac
arrythmia
• Late complication-High voltage injuries-
1-cataract development
2-Progressive nerve degeneration
3-cognitive /psychological impairement
4.
PATHOPHYSIOLOGY
3Forms of electricalinjury-
• Low voltage injuries(<440v),
• High voltage(>1000V),
• ultrahigh(lightning-300,000A)
3 mechanism-
• 1-precipitation of cytoplasmic Protein under the influence of electrical
charge
• 2-Tissue heat generated by passage of current
• 3-Collateral flame burn caused by ignited clothes or electrical flash
5.
FACTORS RESPONSIBLE FORSEVERITY OF
ELECTRICAL BURN
• 1-child susceptibility
• 2-contact point resistance
• 3-contact duration
• 4-current flow pathway
• 5-Current type
• 6-Ameprage
• 7-voltage
6.
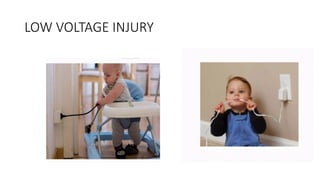
LOW VOLTAGE INJURIES-
•1-Usually d/t biting on an extension cord.
• 2-produce localized burn to the mouths
• 3-Mostly involve portion of upper lip and lower lip
• 4-nonconductive injury
• 5-not requiring hospital admission
• 6-Only topical antibiotics cream used for visible injury
HIGH VOLTAGE INJURY
•1-Mortality rate-3-15%
• 2-Survivors has higher rate of morbidity like major limb amputation.
• Entry and exit site show characteristic features.
• Majority of entry wound in upper extremity with small exit wound in
lower extremity.
• It can cause damage to abdominal viscera , thoracic structures ,
nervous system
• It can manifest as cardiac abnormality , renal abnormality and
compartment syndrome.
LIGHTNING INJURY-
• 1-mostdangerous form
• 2-OCCURS WHEN-
• 1)High voltage current directly strikes a person
• 2)CURRENT STRIKES THE GROUND OR ADJACENT OBJECT.
• Entry ,exit and path lesions are present.
• Internal organ injury along the path is common
• Feathering or arborescent pattern is characteristics
• Linear burns are in the location where sweat is present.
12.
• It canmanifest severe Cardiac ,severe CNS , Severe Renal
complications.
• Lightning burns depend on
• 1-The current path
• 2-The types of clothing worn
• 3-the presence of metal
• 4-cutaneous moisture
CLASSIFICATION OF ELECTRICALBURN-
• 1-True electrical burn-d/t flow of current
• 2- Arc burn-d/t electric arc generated as the current passes from the
source to object
• 3-Flame burn-d/t ignition of clothing and sorroundings
• 4-lightning strike-
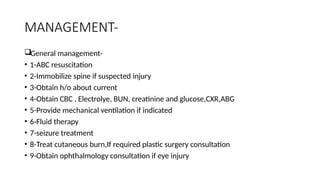
MANAGEMENT-
General management-
• 1-ABCresuscitation
• 2-Immobilize spine if suspected injury
• 3-Obtain h/o about current
• 4-Obtain CBC , Electrolye, BUN, creatinine and glucose,CXR,ABG
• 5-Provide mechanical ventilation if indicated
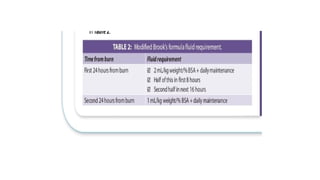
• 6-Fluid therapy
• 7-seizure treatment
• 8-Treat cutaneous burn,If required plastic surgery consultation
• 9-Obtain ophthalmology consultation if eye injury
21.
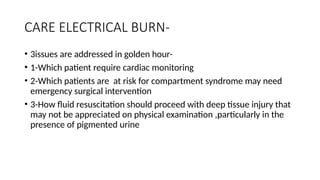
CARE ELECTRICAL BURN-
•3issues are addressed in golden hour-
• 1-Which patient require cardiac monitoring
• 2-Which patients are at risk for compartment syndrome may need
emergency surgical intervention
• 3-How fluid resuscitation should proceed with deep tissue injury that
may not be appreciated on physical examination ,particularly in the
presence of pigmented urine
22.
CARDIAC MONITORING-
• 1-Cardiacdysrhythmia,2-Cardiac arrest,3-myocardial damage can
occur post injury ;requiring cardiac evaluation and cardiac monitoring.
• ECG-Children with electrical injury
• HOSPITALIZED-CHILDREN WITH DOCUMENTED
DYSARYTHMIA,CARDIAC ISCHEMIA OR H/O LOSS OF CONSCIOUSNESS
23.
SURGICAL INTERVENTIONS-
• Requiringemergency surgery-
• 1-Evidence of compartment syndrome
• 2-Evidence of nerve or vessel compression due to edematous
compartment
• 3-On going rhabdomyolysis with myoglobinuria that lead to kidney
failure.
• Escharotomy-for circumferential 3 rd degree burn injuries with tissue
compression and neurovascular compromise.
• Fasciotomies- patient with compartment syndrome and ongoing
myonecrosis or neurovascular compormise
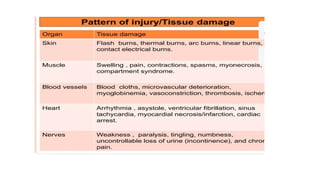
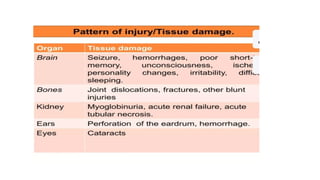
Conclusion-
• Depending onthe current pathway , different organ can get affected
by electrical burn.
• In high voltage electrical injury,ventricular fibrillation,myocardial
damage and cardiac standstill is the common cause of mortality
• No –let go phenomenon ,caused by alternate current may cause
violent muscle contraction and lung bone fracture.
• Compartment syndrome is caused by deep tissue electrical
burns ,require early identification and surgical interventions as
fasciotomy and /or early debridement for affected extremity salvage.
31.
PREVENTION-
• 1-Electrical outletsafety cover
• 2-Keeping the electrical appliances beyond the child :s reach.
• 3-Not using electrical gadgets in bath/Shower


















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)










