ATLS protocol
1. Immediatelylife-threatening conditions are identified and
emergency management begun.
2. A. Airway maintenance with cervical spine control
3. B. Breathing and ventilation
4. C. Circulation with haemorrhage control
5. D. Disability - neurological status
6. E. Exposure + environmental control.
4.
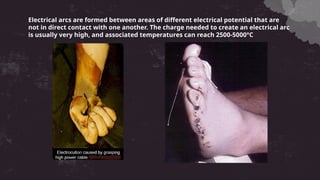
Electrical arcs areformed between areas of different electrical potential that are
not in direct contact with one another. The charge needed to create an electrical arc
is usually very high, and associated temperatures can reach 2500-5000°C
9.
TABLE OF CONTENTS
ATLSProtocol Resuscitation
01 02
Electrocardiograp
hic monitoring
Wound Care
03 04
10.
Resuscitation
Burn resuscitation formulasbased on body
surface area burned inaccurate
In absence of gross myo/hemoglobinuria, goal
of resuscitation is to maintain normal vital
signs and a urine output of 30–50 mL/h with
Ringer’s lactate (rate adjusted on an hourly
basis)
Presence of pigmented(darker than light pink) urine
Myoglobin and hemoglobin pigments
Rapid, osmotic diuresis with initial alkalinization to minimize
pigment precipitation in renal tubules
Loop diuretics are not as efficient as mannitol.
Required U/O very high for several hours following injury,
followed by significant reduction (venous return from the injured
part to the central circulation is thrombosed)
Indications for cardiacmonitoring
Cardiac arrhythmia on
transport
Documented cardiac arrest
Abnormal EKG in ER (other than
sinus brady- or tachycardia)
Burn size or patient age
would require monitoring
15.
Electrocardiographic
monitoring
● Most commonabnormalities seen on
an electrocardiogram (ECG) are sinus
tachycardia, nonspecific ST- and T-wave
changes, heart blocks, and
prolongation of the QT interval
● Creatine kinase (CK) and MB creatine
kinase (CK-MB) levels are poor
indicators of myocardial injury in the
absence of ECG finding of myocardial
damage
16.
Wound care
Cleaning thewound- saline, soap and
water, or chlorhexidine 0.1%
solution
Local burn care is performed using
mafenide acetate (Sulfamylon) on
the thick eschar of the contact
points (excellent penetration).
Silver sulfadiazine is used for microbial
control on the deep flash/flame
components
Biologic dressing used on more
superficial areas
Elevation- to limit swelling
17.
● Surgical excisionbegun 2–3 days postburn
● Obviously necrotic tissue removed, while
tissues of questionable viability are retained
and re-evaluated every 2–3 days until wound
closure
● Conservative course of tissue removal and
wound closure with a combination of skin
grafts and/or flaps
● Ongoing program of physical therapy and
functional splinting
18.
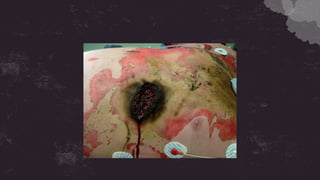
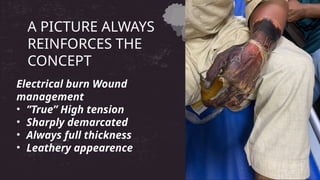
Electrical burn Wound
management
•”True” High tension
• Sharply demarcated
• Always full thickness
• Leathery appearence
A PICTURE ALWAYS
REINFORCES THE
CONCEPT
19.
Accurate predictors oftissue damage
Radionuclide scanning with xenon-133
Technetium pyrophosphate.
Gadolinium-enhanced MR imaging
MPLES
Scalp burn
Sparing galea:-
-Excisionand skin grafting directly onto the galea
Penetrate outer table of skull or deeper:-
-Removing dead bone with an osteotome or a dental type
burr.
-Drilling multiple holes in a close set pattern, deep enough to
cause bleeding from viable cancellous bone
(patient’s advanced age or large burn size precludes more
aggressive approaches to wound closure)
22.
Scalp burn
-Rotation scalpflap(s) over the burned area. Split-
thickness skin grafts over donor defect.
-This provides rapid closure and is associated with minimal
morbidity
-Skin expansion of the hair-bearing area can be performed
12–18 months
-Larger scalp defects are closed with free flaps
23.
thoracic injury tothe deep
structures phrenic nerve and
direct thermal injury to the
heart
present special closure problems
(adjacent or remote soft tissue
flaps) for coverage of exposed
bone and cartilage.
Costal chondritis is the most
frequent complication of deep
chest wall burns requiring
multiple debridements
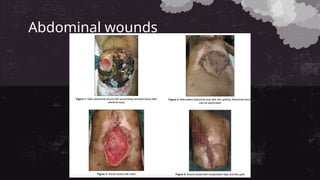
Chest wall injuries
-Internal injuries bothdirectly under
contact points and remotely as
result of late ischemic necrosis
-Patients must be frequently evaluated
for changes in their abdominal
examination and/or feeding
tolerance.
-Deterioration mandates laparotomy.
-Repair of large abdominal wall
wounds
Chest wall injuries
27.
Younger children
only theoral commissure are initially
treated very conservatively
most serious complication is bleeding
from the labial artery (10–14 days
after injury)
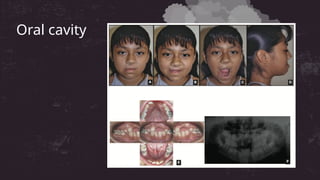
Oral cavity
28.
Gentle stretching andthe use of oral splints give good
cosmetic and functional results in most patients
Severe mircostomia is corrected by mucosal advancement
flaps.
Burns of the mid-portions of mouth heal very poorly and
require a much more aggressive surgical approach with
carefully planned reconstruction
Oral cavity
Compartment syndrome
First 48hours post injury in high voltage injury
Damaged muscle, swelling within the investing fascia of the
extremity
Loss of pulses is one of the last signs
Serial examinations of the affected extremities or repeated
measurements of compartment pressures
33.
Compartment syndrome
Indications forfasciotomies
clinical signs of compartment syndrome,
Progressive nerve dysfunction
failure of resuscitation with other patients undergoing
exploration
aggressive debridement on the third to fifth postburn day
34.
Surgical Indications
Fasciotomy forcompartment syndrome
Escharotomy for full-thickness circumferential
burns
Early exploration & debridement of necrotic tissue
Amputation when limb is non-viable