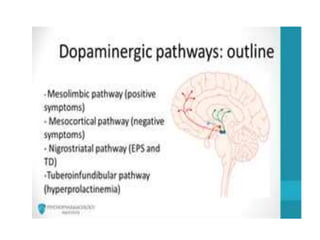
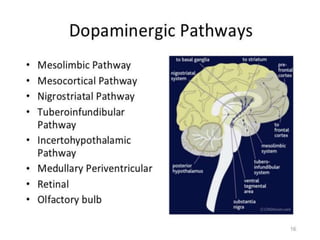
This document discusses neuropsychiatry and antipsychotic medications. It begins by outlining the four dopamine pathways relevant to antipsychotic pharmacology: mesolimbic, mesocortical, nigrostriatal, and tuberoinfundibular. It then describes each pathway's anatomy, physiology, and implications for symptoms of schizophrenia. The document also covers types of antipsychotics, their mechanisms of action, indications, and various adverse effects including weight gain, sedation, and neurological side effects. In summary, it provides an overview of the neurobiology underpinning antipsychotic treatment and the therapeutic and adverse impacts of blocking different dopamine pathways in the brain.



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










