Downloaded 1,309 times
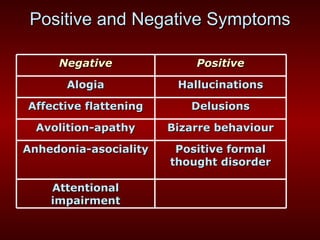

The document provides information about schizophrenia, including its definition, symptoms, diagnosis, course, treatment, and etiology. Some key points: - Schizophrenia is defined by positive and negative symptoms that last at least 6 months and cause deterioration in functioning. - It affects about 1% of the population and typically emerges in late adolescence/early adulthood. - Symptoms include hallucinations, delusions, disorganized speech and behavior, emotional blunting, and lack of motivation. - Treatment involves antipsychotic medication and psychosocial support like therapy. The exact causes are unknown but are thought to involve genetic and environmental factors impacting brain development.

































































































