

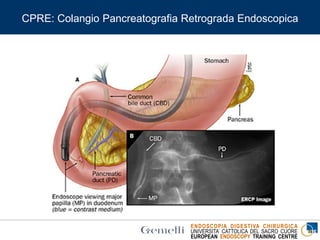
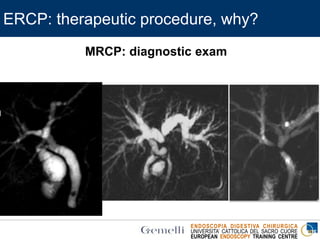
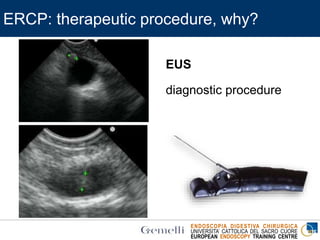
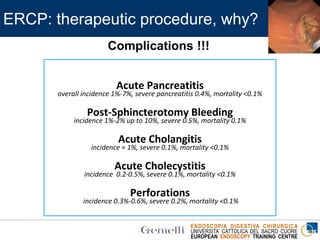
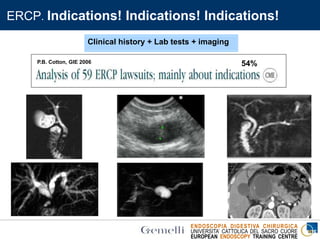
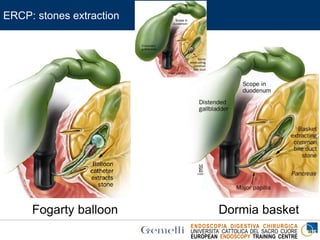
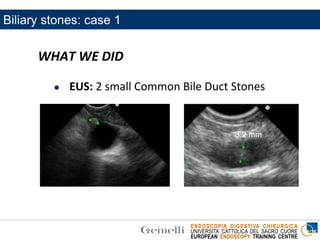
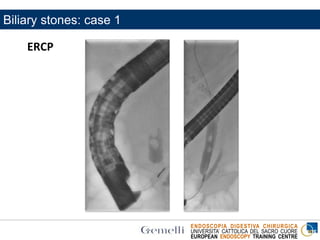
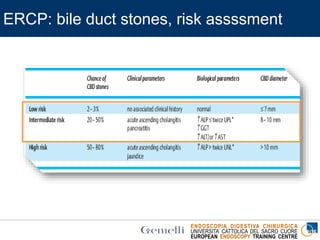
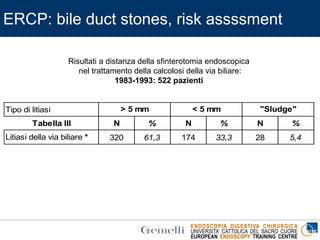

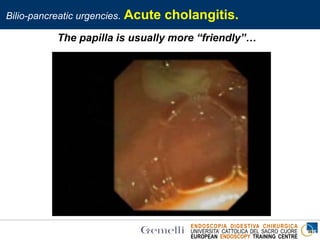
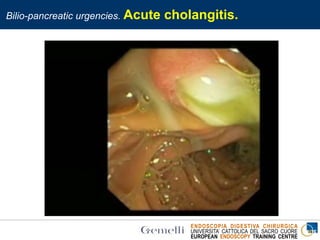
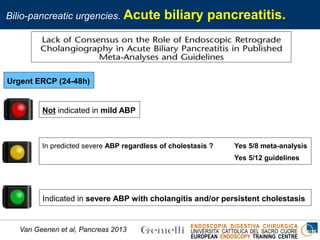
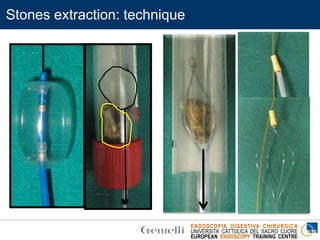
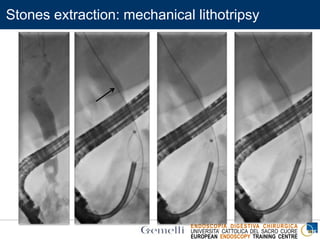
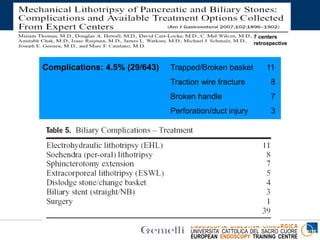

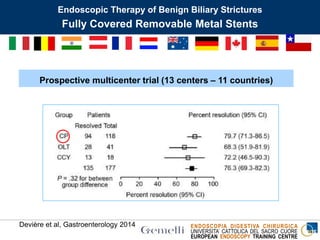
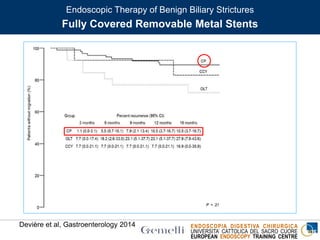
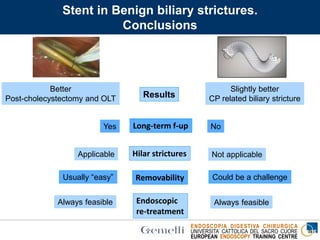
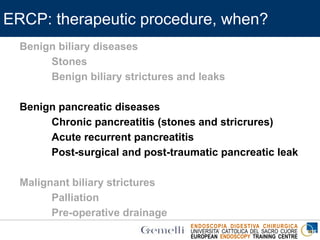



The document discusses endoscopic procedures for managing biliary and pancreatic diseases, emphasizing the role of ERCP (Endoscopic Retrograde Cholangiopancreatography) as a therapeutic method. It details indications for ERCP, various complications, and specific cases involving patients with biliary stones. Additionally, it evaluates techniques for stone extraction and the importance of early biliary drainage in acute conditions like cholangitis and biliary pancreatitis.

































![[OWASP-TR Mobil Güvenlik Çalıştayı 2015] Sertel Şıracı - Mobil Uygulama Güven...](https://cdn.slidesharecdn.com/ss_thumbnails/sertelsiraci-mobiluygulamaguvenligivehukuk-151109072048-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[OWASP-TR Mobil Güvenlik Çalıştayı 2015] Mehmet Sabır Kiraz & Osmanbey Uzunko...](https://cdn.slidesharecdn.com/ss_thumbnails/mehmetsabrkirazosmanbeyuzunkol-kriptografikhesaplamalarnbulutaguvenlitevdisi-151109072324-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













