



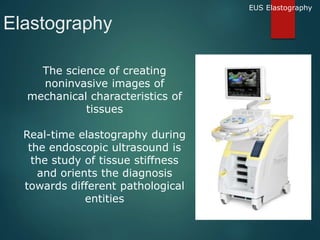
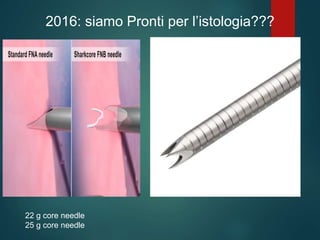
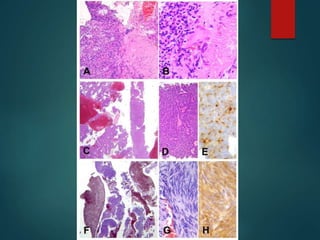



The document discusses innovations in endoscopic ultrasound (EUS) and its applications in oncology, highlighting the development of EUS techniques and the importance of histology for cancer diagnosis. It reviews advancements in contrast-enhanced EUS and elastography, emphasizing their roles in improving diagnostic accuracy and guiding treatment decisions. Additionally, it addresses the challenges and future directions of EUS-based techniques, including the need for adequate tissue samples for molecular analysis.























































































