Downloaded 1,049 times
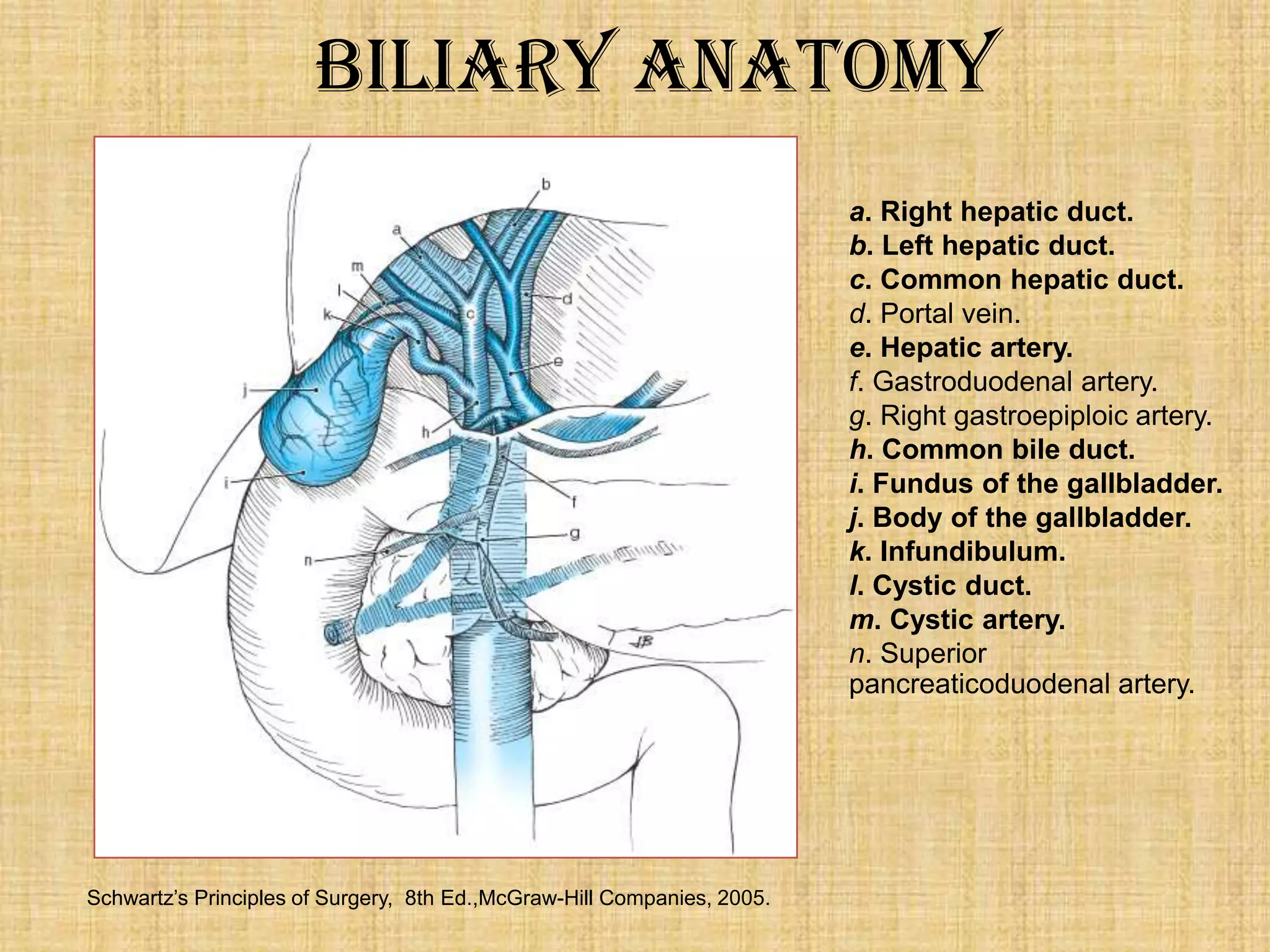
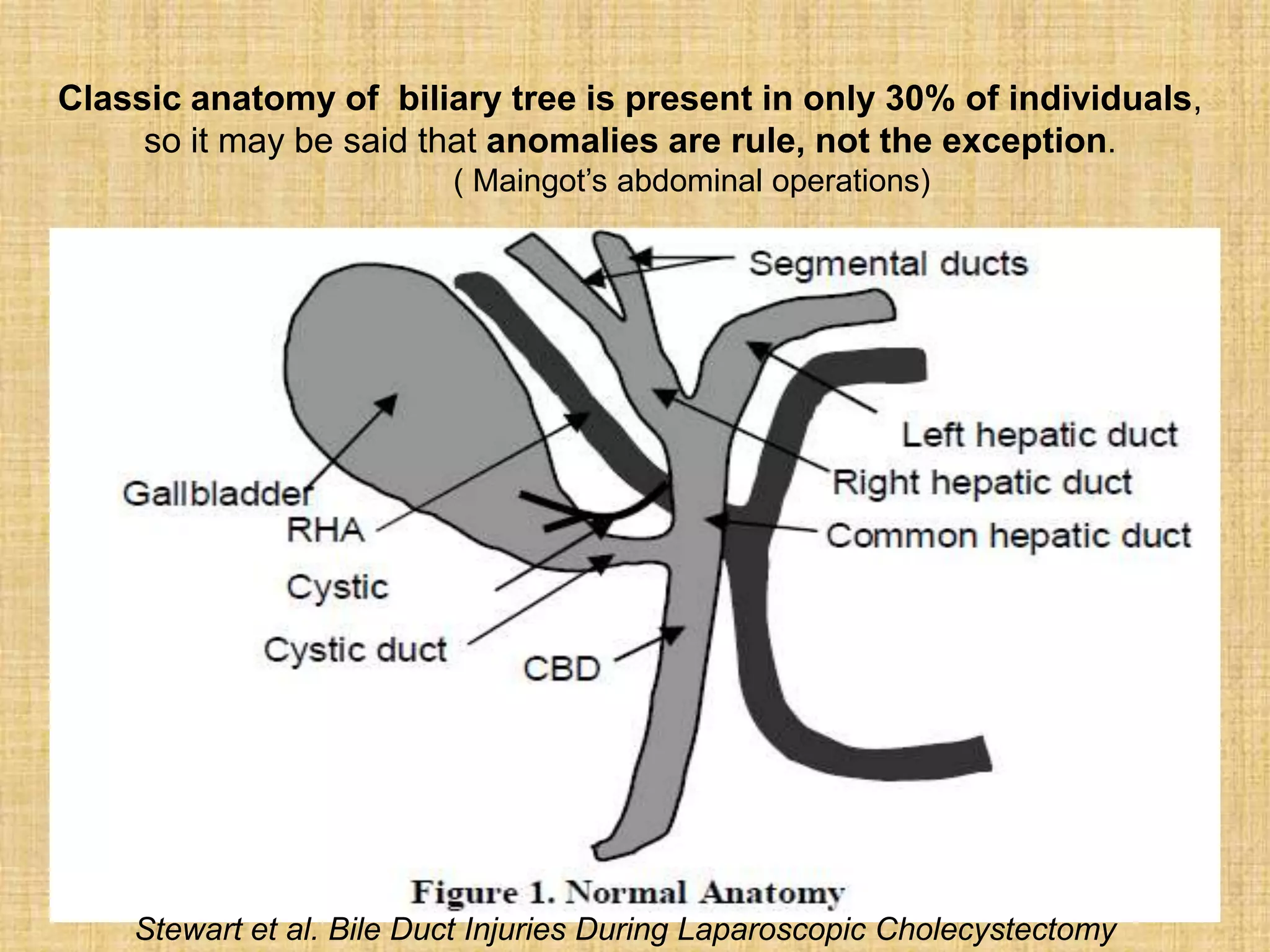
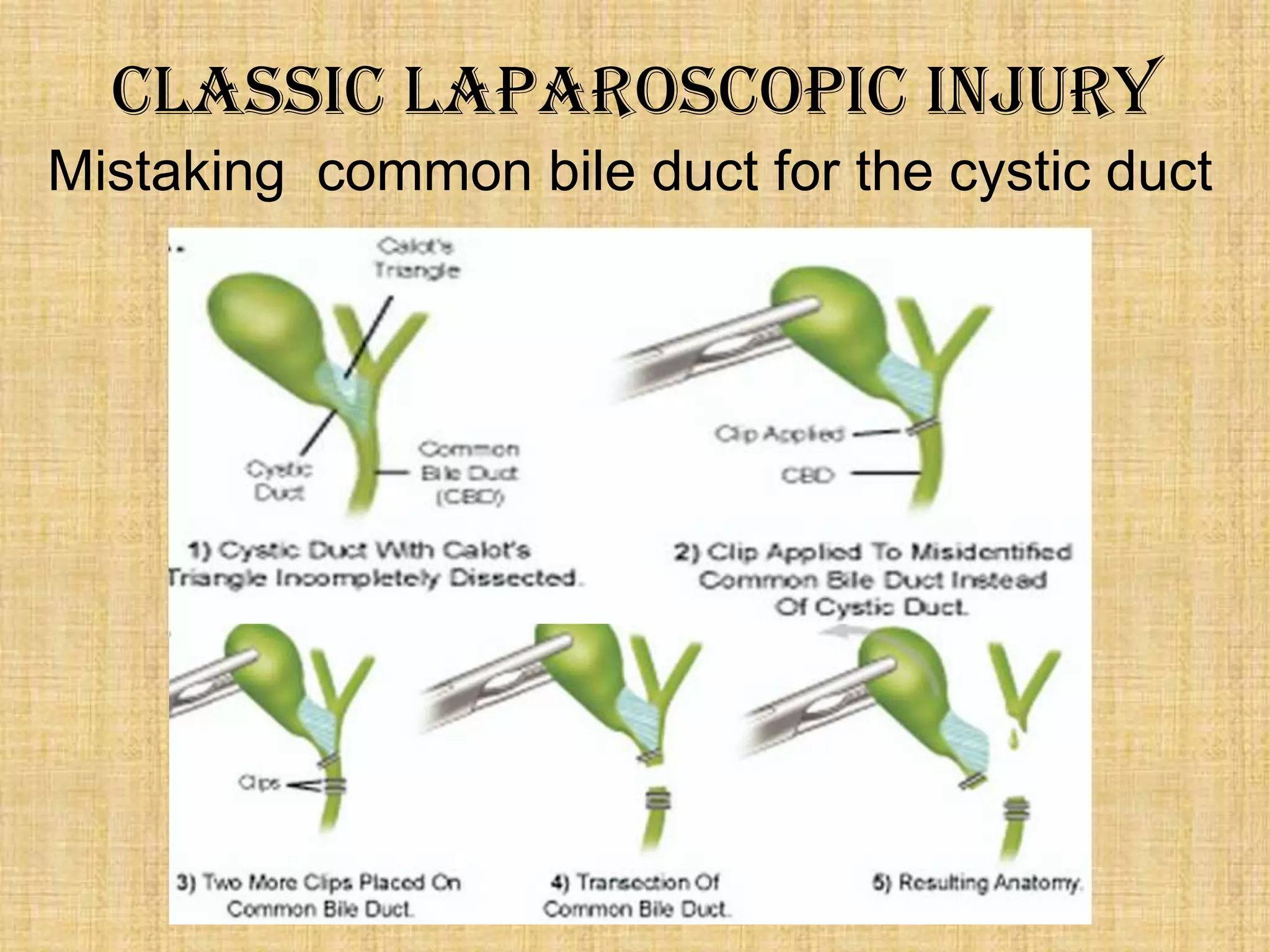
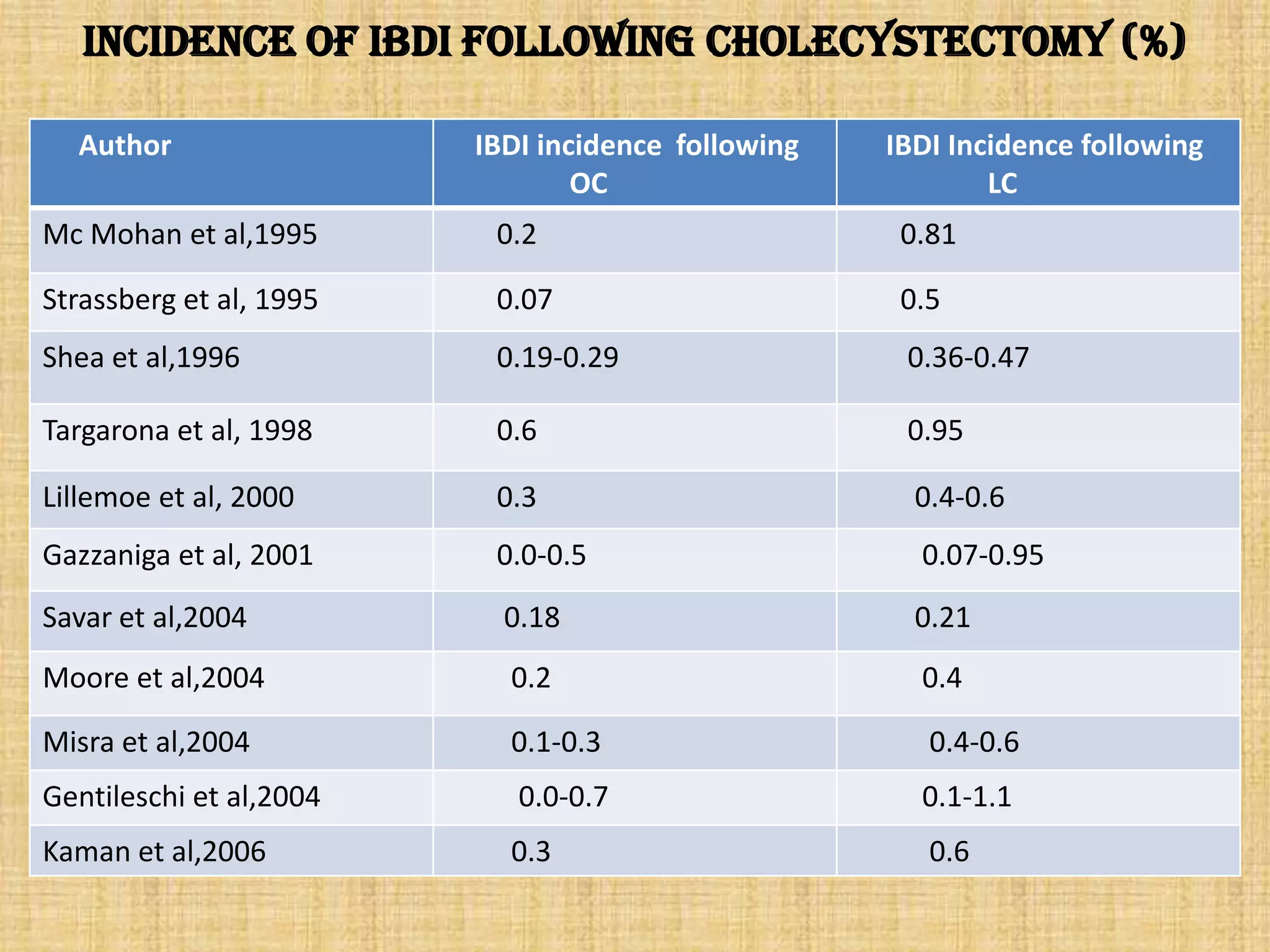
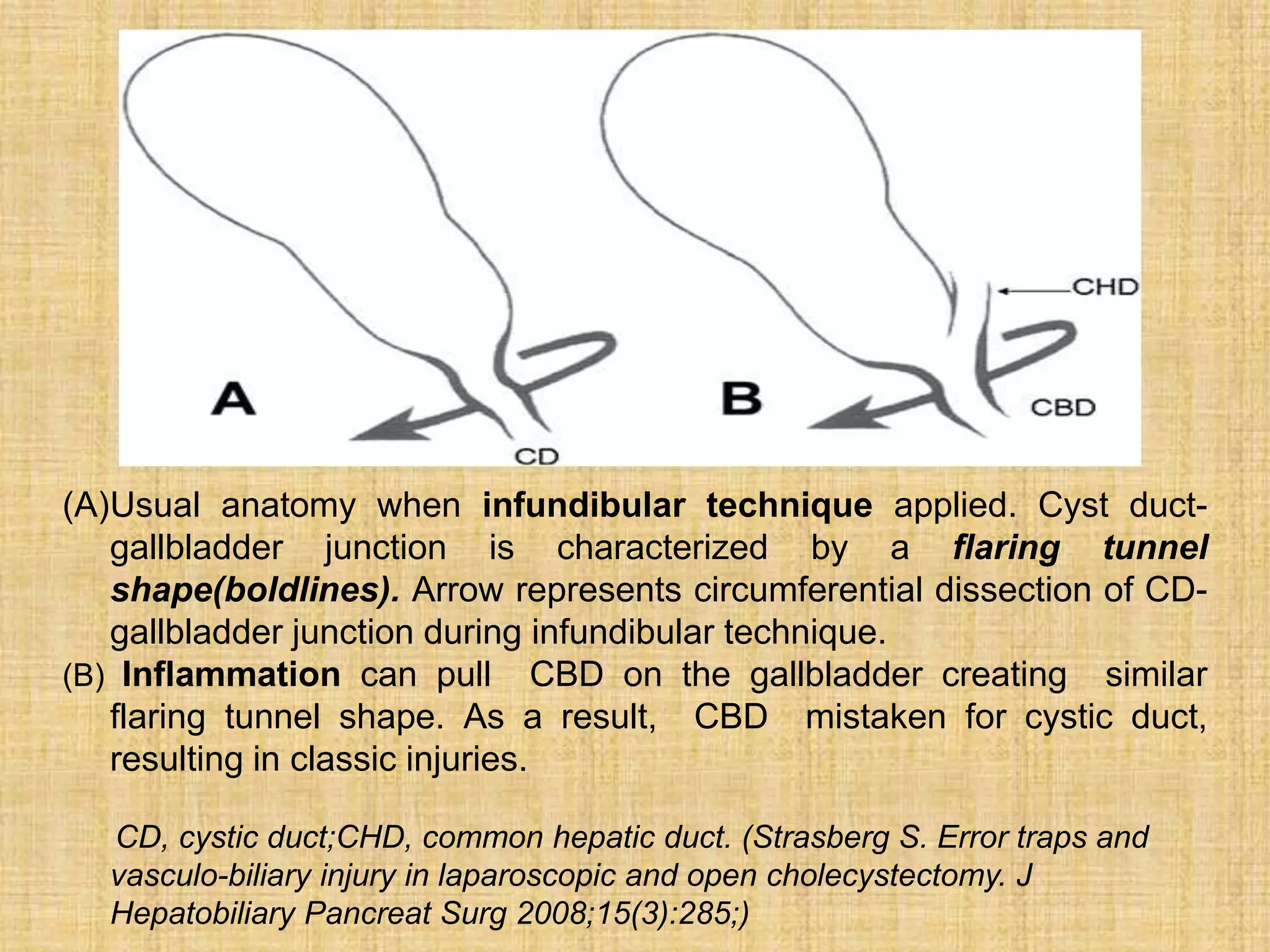
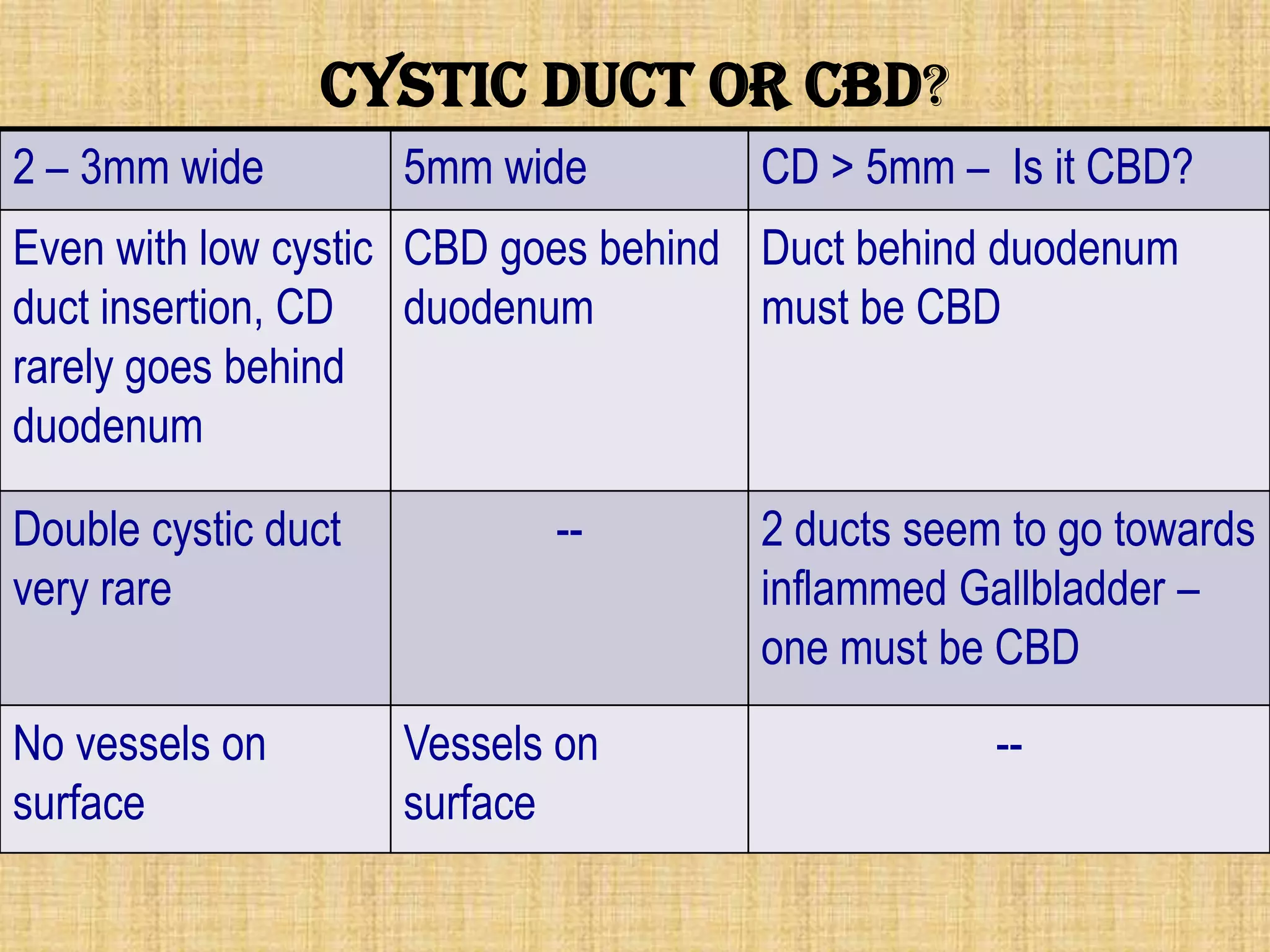
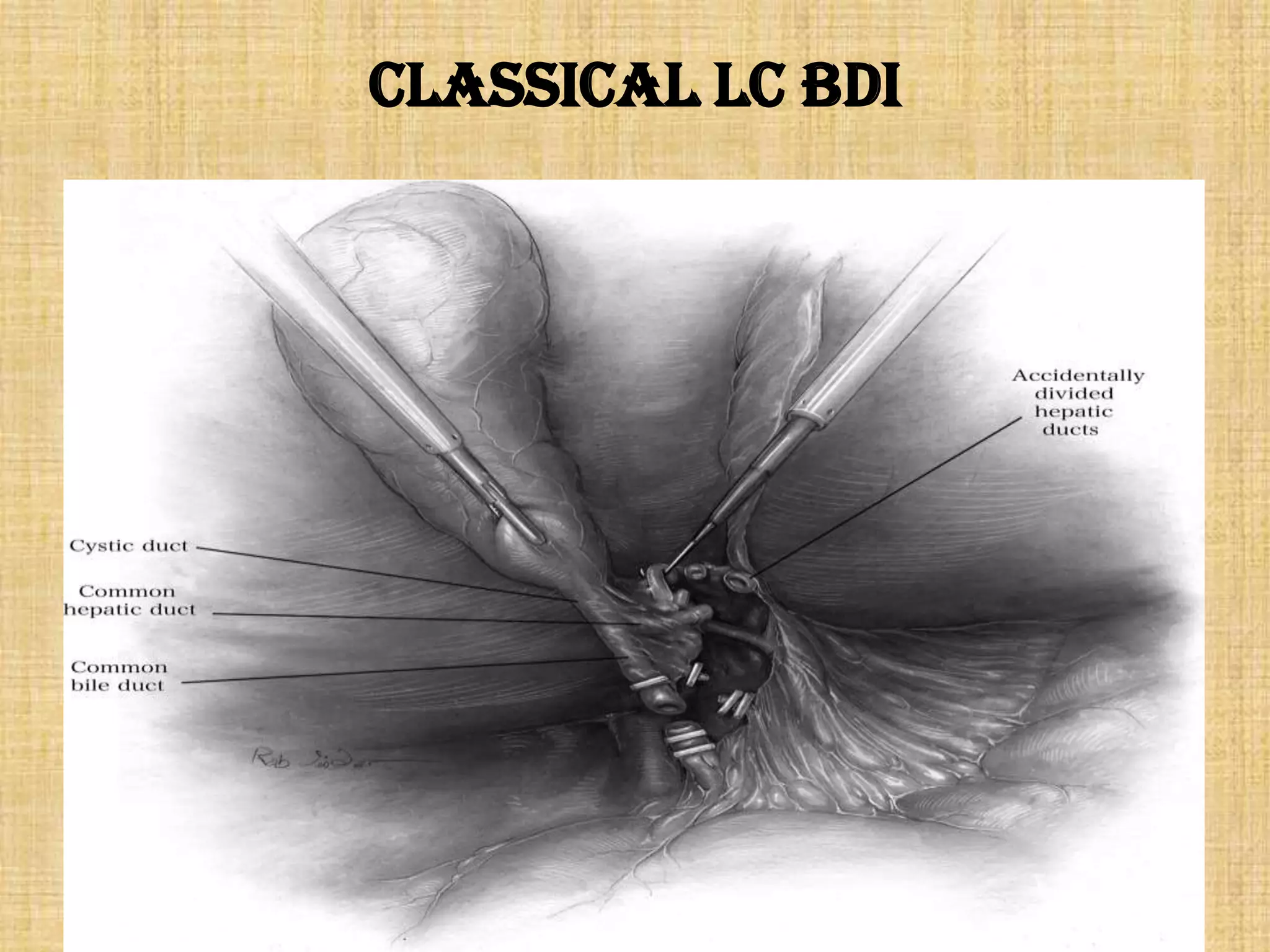
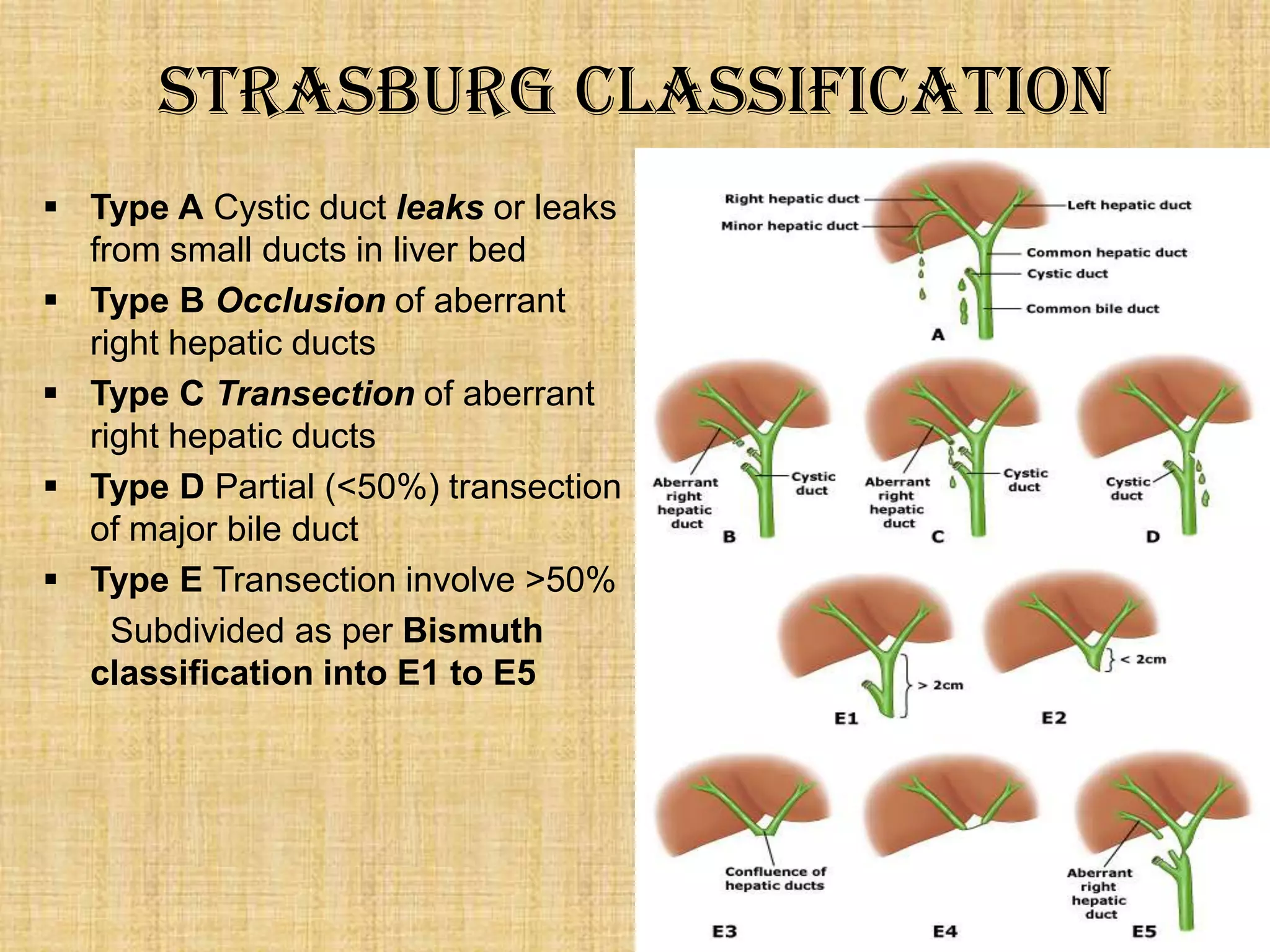


The document discusses biliary injuries during laparoscopic cholecystectomy, detailing historical milestones, anatomical considerations, and complications associated with the procedure. It highlights risk factors for bile duct injuries, emphasizing the learning curve for surgeons and the increase in injury rates since the adoption of laparoscopic methods. The text also outlines prevention strategies and management approaches for such injuries, advocating for careful identification of biliary structures during surgery.




















































































