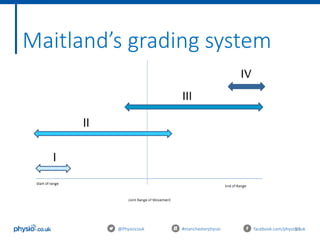
This document outlines an introduction to basic joint mobilizations for sports and massage therapists. It includes the itinerary for the workshop, which involves learning the theory of joint mobilizations, practicing assessments, and practicing different joint mobilization techniques. The document covers topics such as the definition of a joint mobilization, anatomy of synovial joints, types of synovial joints, physiological and accessory joint movements, assessment of range of motion and end feels, contraindications to joint mobilizations, and Maitland's grading system for joint mobilizations.