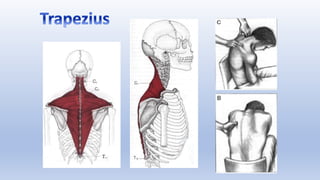
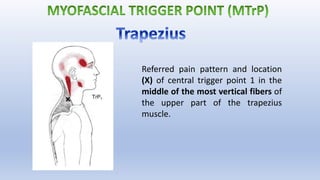
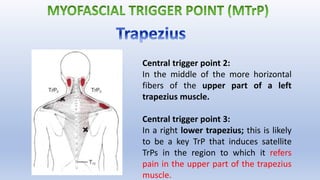
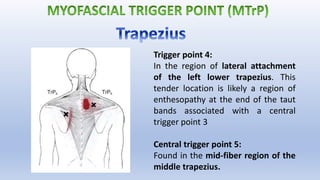
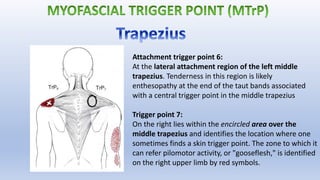
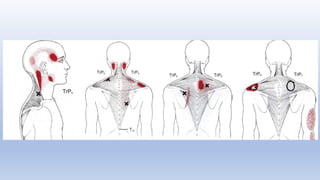
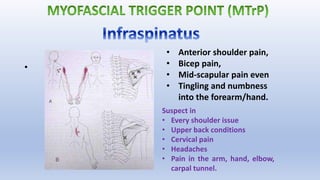
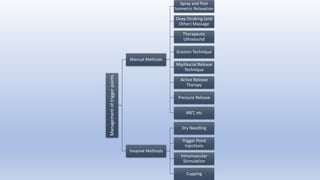
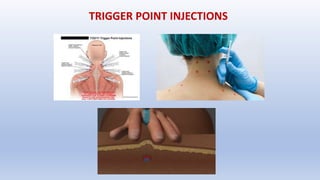
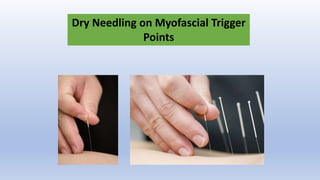
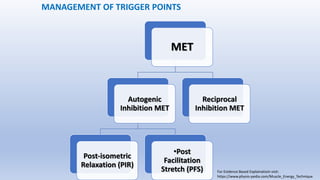
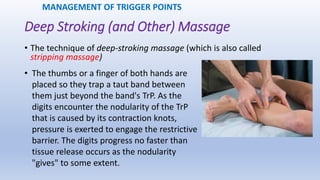
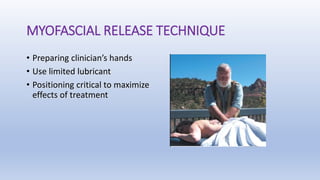
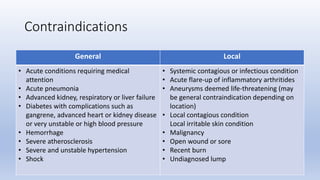
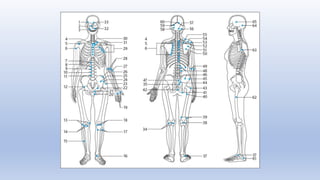
This document discusses trigger points and their management. It identifies 7 central trigger points located in different areas of the trapezius muscle that can refer pain to other areas. It then lists various manual and invasive techniques for managing trigger points, including dry needling, trigger point injections, massage, pressure release and myofascial release. Guidelines are provided for techniques like trigger point pressure release. Precautions, contraindications and potential side effects of trigger point treatment are also outlined.