






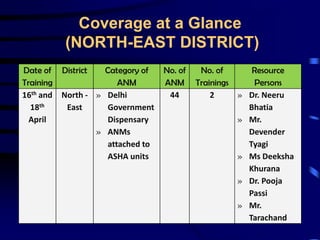
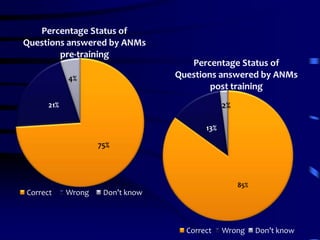
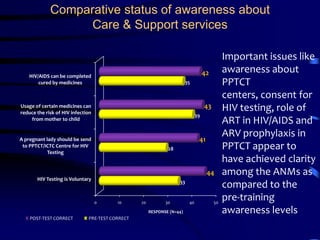

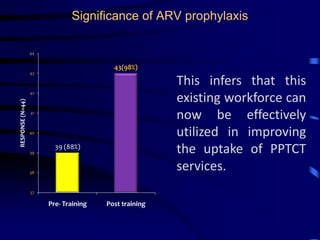
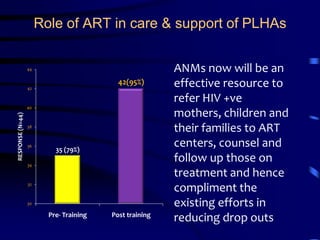


The document outlines a training project conducted by Astron Hospital and Healthcare Consultants to educate Auxiliary Nurse Midwives (ANMs) in Delhi on HIV/AIDS awareness and integration with reproductive and child health services. The training included various sessions on HIV basics, stigma, and care strategies, leading to improved knowledge and referral capabilities among ANMs regarding HIV services. Recommendations for future training emphasize ongoing education and practical field visits to strengthen knowledge and service delivery integration.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



