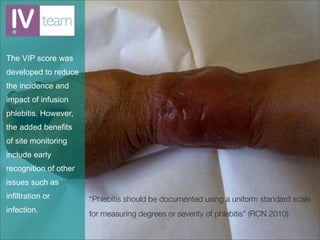
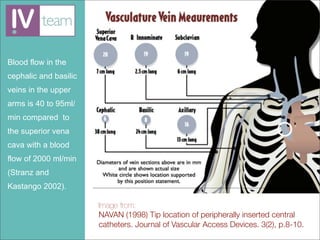
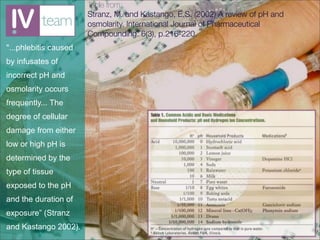
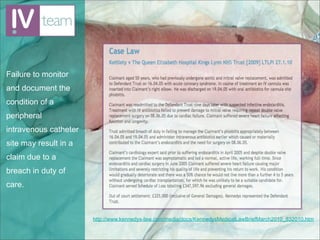
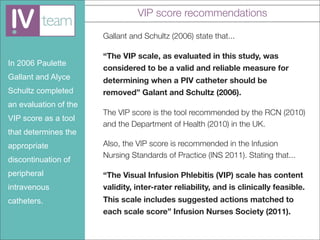
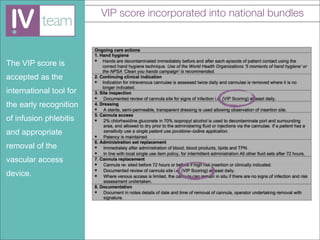
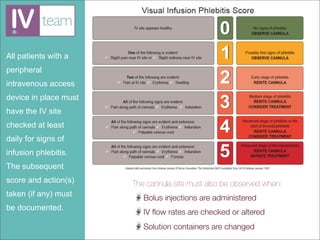
The document discusses the importance of regular evaluation and monitoring of intravenous (IV) sites to enhance patient safety and prevent complications such as infusion phlebitis. It emphasizes the use of the Visual Infusion Phlebitis (VIP) score as a validated tool for assessing IV site conditions and guiding necessary actions. Recommendations include daily checks of IV sites and documentation of any changes or actions taken to manage potential phlebitis.