
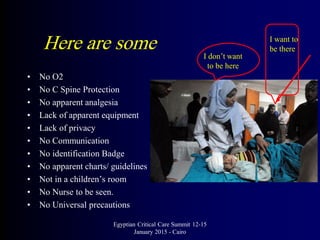













The document outlines quality indicators in emergency medicine presented by Ahmed Kamal at the Egyptian Critical Care Summit in Cairo, emphasizing the importance of unbiased performance analysis and effective emergency care delivery. Key indicators discussed include waiting times, pain control, and patient communication, alongside challenges faced by emergency departments. Recommendations for improvements include adequate staffing and resource allocation to enhance patient experience and safety.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


