Downloaded 324 times



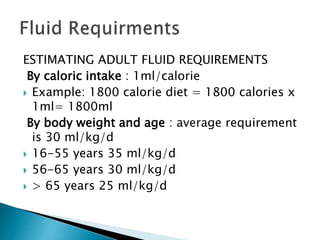
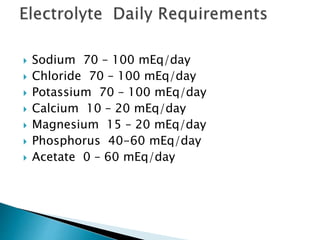
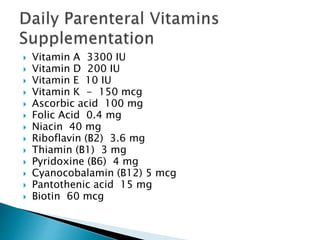
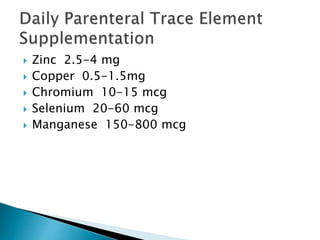


Human nutrition is vital for health, requiring essential nutrients from the diet, including macronutrients and micronutrients. Nutritional assessment is crucial for patients at risk of malnutrition due to illness or dietary changes, and both enteral and parenteral nutrition are important for those unable to meet their nutritional needs. Specialized nutritional support can improve patient outcomes, but should be used judiciously, balancing benefits and risks.























































































