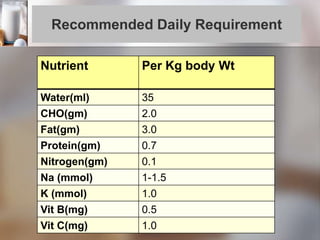
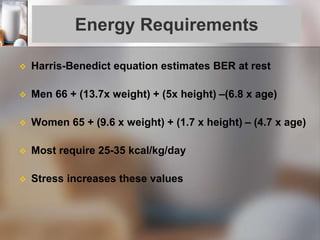
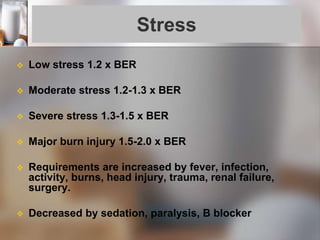
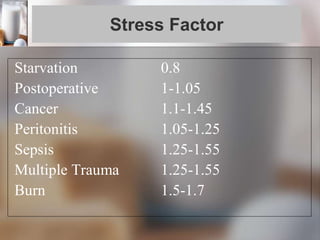
This document discusses nutritional support for surgical patients. It defines nutritional support as the provision of nutrients orally, enterally, or parenterally to maintain or restore optimal nutrition and health. Patients who cannot meet nutrient requirements or have inadequate oral intake may need support. Evaluation of nutritional status includes assessing weight loss, serum markers, and physical signs. Enteral nutrition via feeding tubes is preferred when possible as it maintains gut function, but parenteral nutrition is needed when the GI tract is nonfunctional or unavailable. Both methods require calculating energy and nutrient needs and monitoring for complications.










































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















