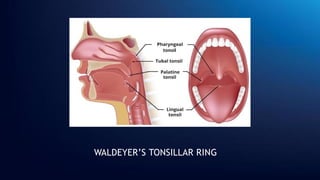
The document provides an overview of acute tonsillitis, detailing the anatomy and function of the tonsils, the etiology and types of the condition, and associated symptoms and signs. It highlights the diagnosis and management of acute tonsillitis, including treatment options and potential complications. The document also touches upon differential diagnoses related to tonsillitis.