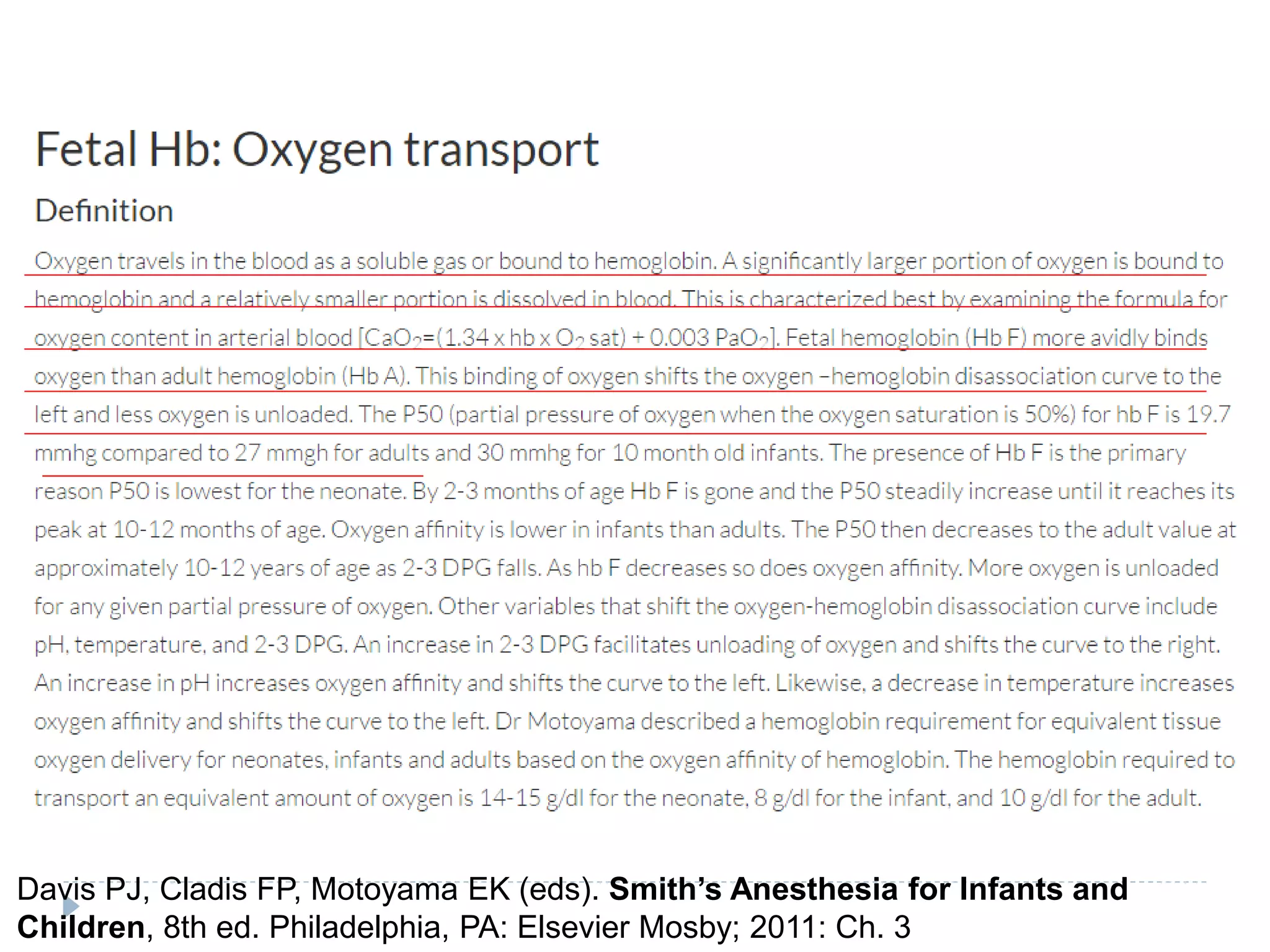
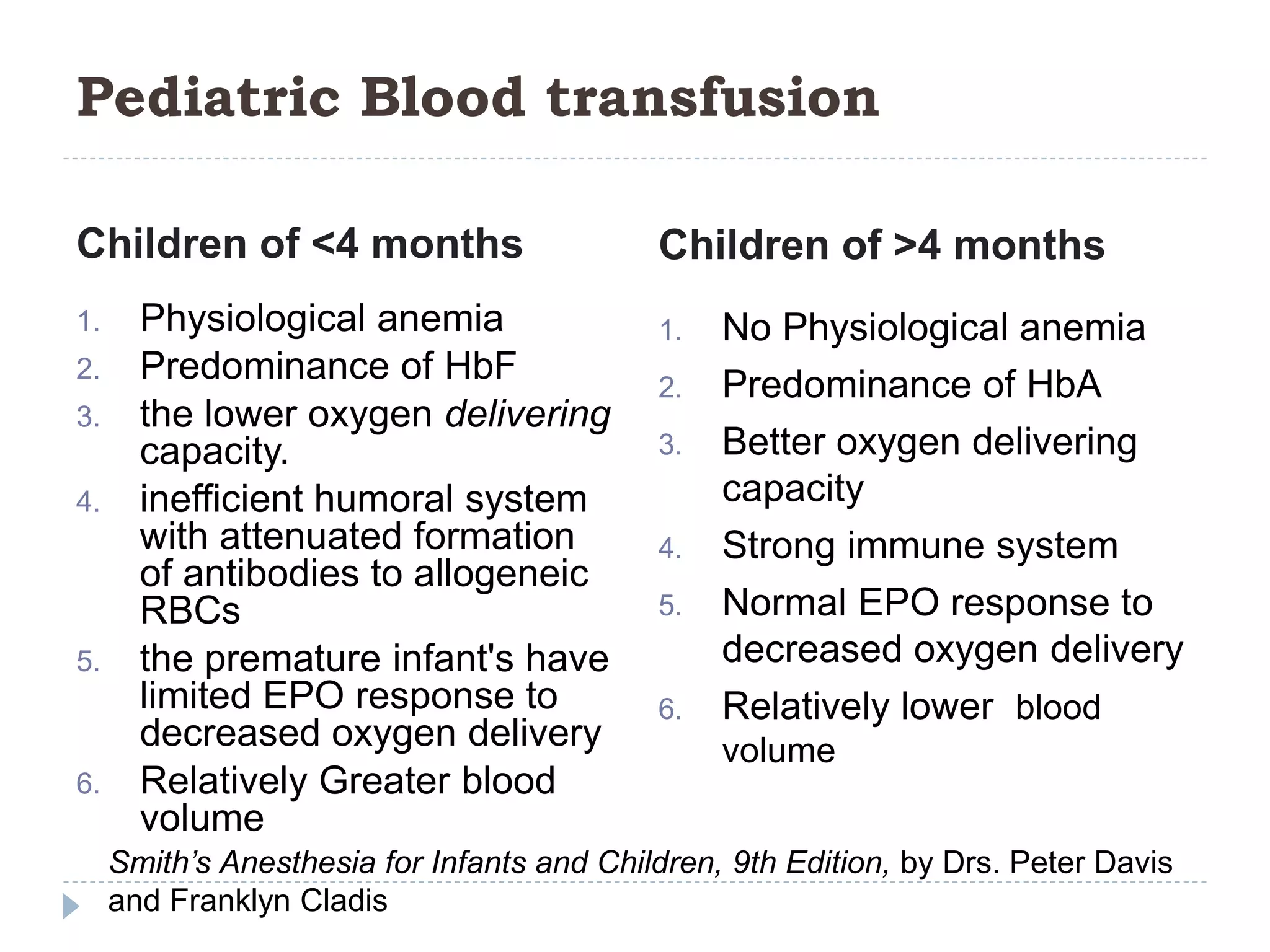
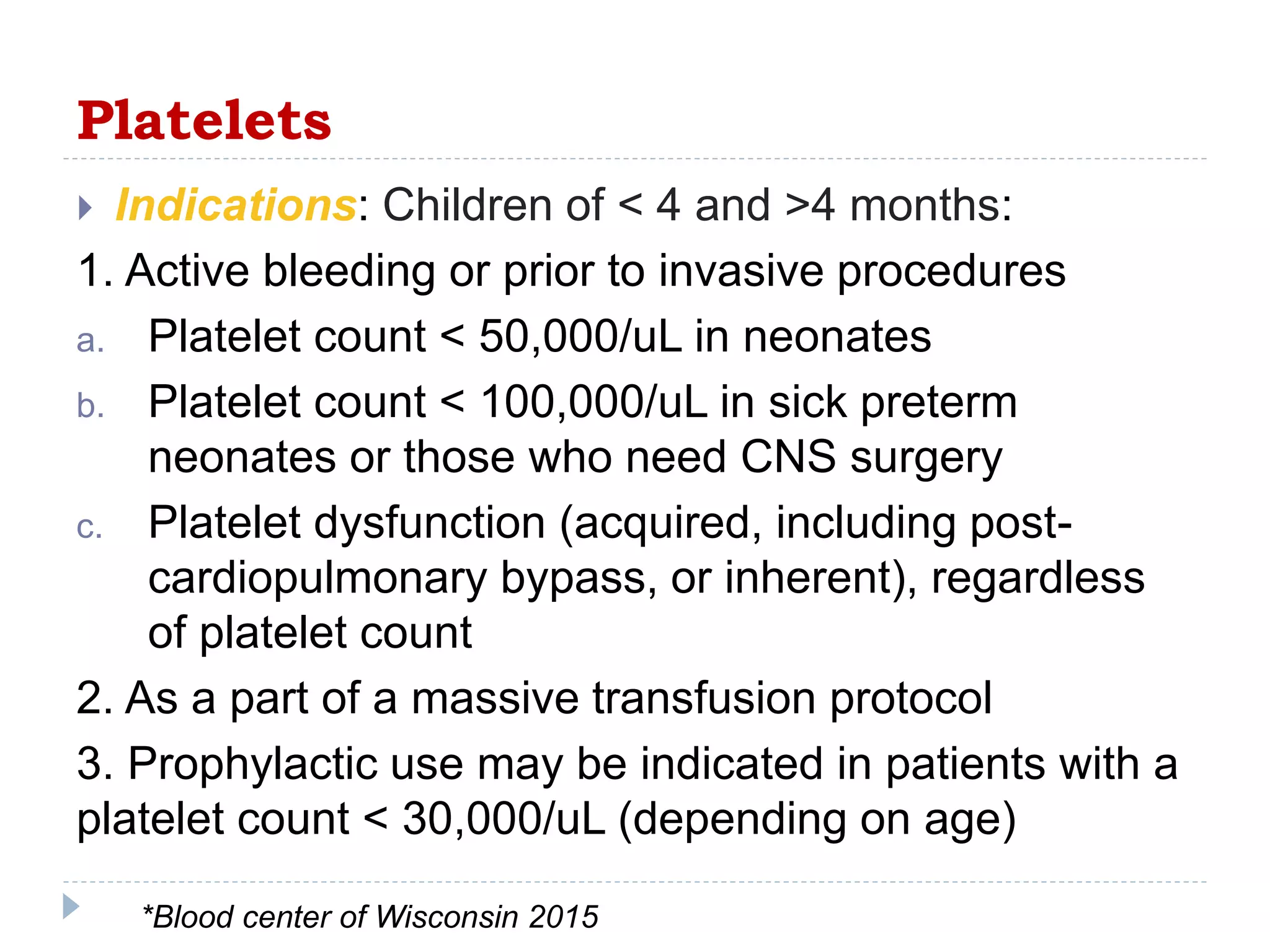
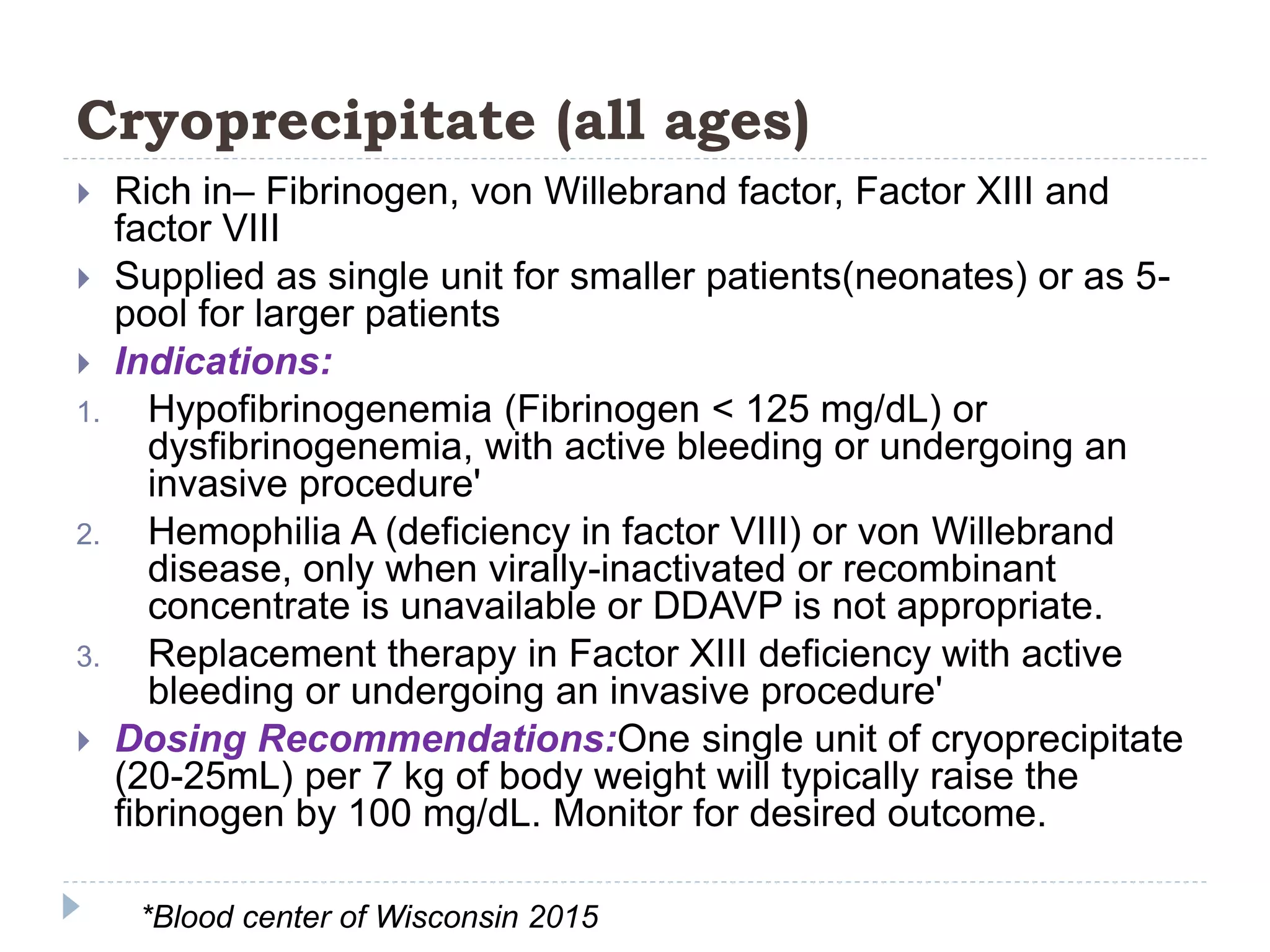
This document provides information about blood transfusions in the pediatric population. It discusses the history of blood transfusions and discoveries such as different blood groups. It outlines the indications and dosing recommendations for transfusing red blood cells, platelets, and plasma in children under 4 months and over 4 months of age. The key points are that transfusions may be needed to treat anemia, bleeding, or other conditions depending on the child's hematologic values and clinical status. Dosing is based on the child's weight and intended to raise hemoglobin, platelet count, or coagulation factors to desired levels.

![Pediatric age group
From birth to 18 years of age [IAP]
up to the age of 21 [U.S. FDA]](https://image.slidesharecdn.com/totransfuse-170824005741/75/To-transfuse-2-2048.jpg)


![Human Blood Group Systems
The term human blood group systems is defined by International
Society of Blood Transfusion as systems in the human species
where cell-surface antigens—in particular, those on blood cells—are
"controlled at a single gene locus or by two or more very closely
linked homologous genes with little or no observable recombination
between them",[1]
It includes the common ABO and Rh- (Rhesus) antigen systems, as
well as many others; thirty-five major human systems are identified
as of November 2014.[2]
ABO blood groups were discovered by Landsteiner in 1901 Later on
Rhesus blood groups were discovered by Landsteiner and Wiener in
1940. [3]
1. ISBT (2016). "International Society for Blood Transfusion (ISBT) Committee on Terminology for
Red Cell Surface Antigens, Terminology Home Page". Retrieved 20 February 2016
2. ISBT (2014). "Table of Blood Group Systems v4.0 (November)" (PDF). International Society
of Blood Transfusion. Retrieved 19 February 2016
3. Landsteiner K, Wiener AS (1940). An agglutinable factor in human blood recognized by immune sera for
Rhesus blood. Proc. Soc Exp. Biol. Med. 43:223-224.](https://image.slidesharecdn.com/totransfuse-170824005741/75/To-transfuse-5-2048.jpg)













![Blood grouping and crossmatching
Blood grouping
The most fatal of all transfusion-related reaction is ABO
incompatibility causing complement-mediated intravascular
hemolysis. Hence, correct blood grouping and typing, and cross-
checking with the blood requisition form is of utmost importance.
ABO typing is carried out by testing RBCs for the A and B antigens
and the serum for the A and B antibodies before transfusion. The
next step involves Rh typing with only 15% of the population being
Rh-negative.
Cross-matching
Cross-matching involves mixing of donor RBCs with the recipient
serum to detect fatal reactions. [19] . Among the three phases, the first
two phases are more important as they detect those involved in fatal
HTR. The total time taken for all the three phases is in between 45
and 60 min.
Mitra R, Mishra N, Rath GP. Blood groups systems. Indian J Anaesth 2014 [cited 2017 Feb
10];58:524-8.
Miller RD. Transfusion therapy. In: Miller RD, ErikssonLI, Fleischer LA, Wiener-
Kronish JP, Young LA, editors. Miller's Anesthesia. 7 th ed. Philadelphia: Churchill
Livingstone Elsevier; 2010. p. 1739-66.](https://image.slidesharecdn.com/totransfuse-170824005741/75/To-transfuse-28-2048.jpg)