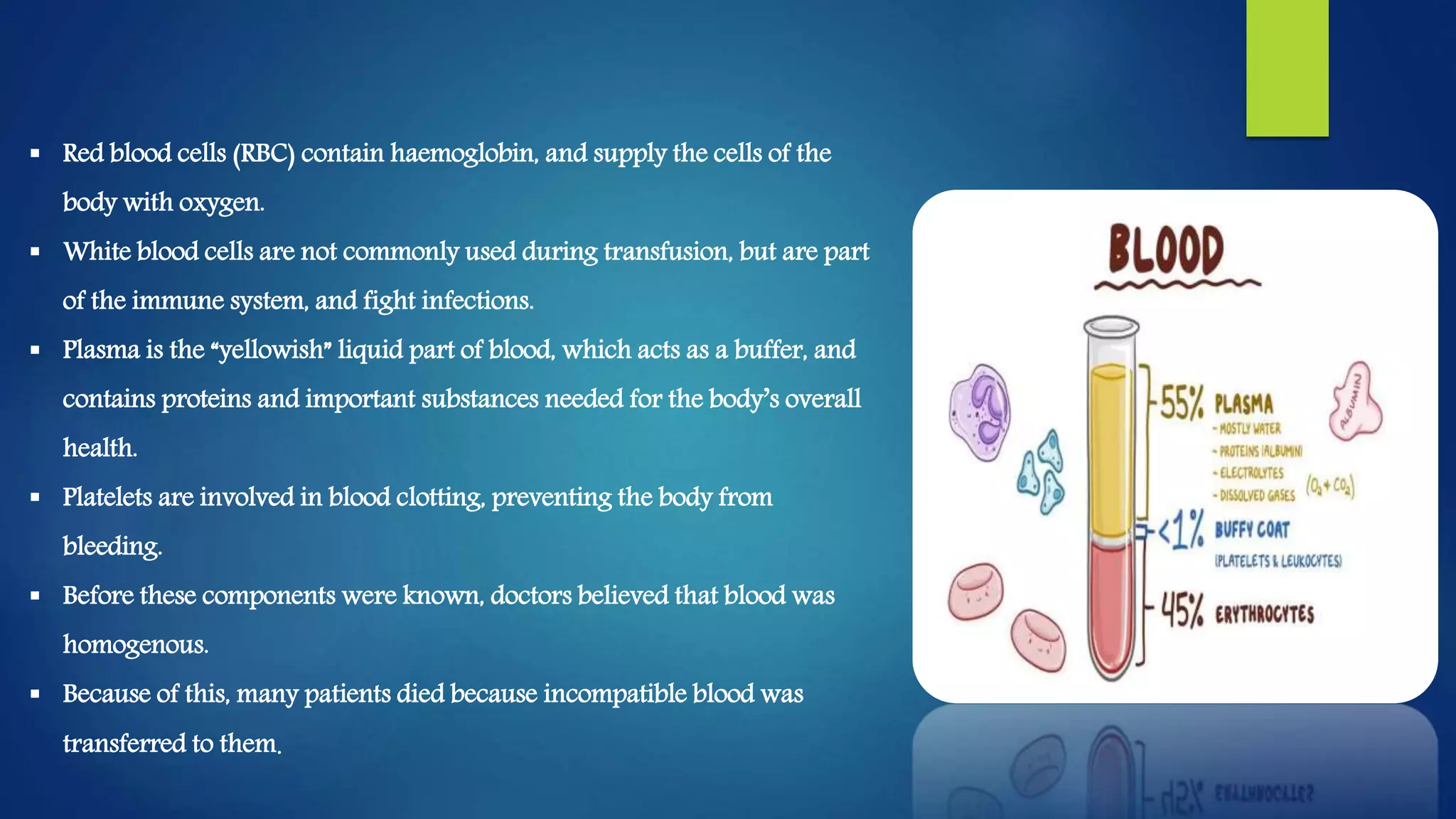
Blood transfusion is a medical procedure where blood or blood components are transferred from one person into the circulatory system of another. There are several types of blood transfusion including allogeneic where the donor and recipient are different people, and autogenic where a person receives their own previously donated blood. The blood transfusion procedure involves verifying the blood type, obtaining consent, administering the transfusion, and monitoring for any complications. Potential complications include transfusion reactions if the blood is mismatched, infections transmitted through the blood, and issues that can arise from using faulty techniques or giving massive amounts of blood.