Downloaded 776 times


![COMPOSITION OF BLOOD
Blood
Cells (45%)
Erythrocytes
[5
million/cumm]
Leucocytes
[4000 – 11000/
cumm]
Agranulocytes Granulocytes
Thrombocytes
[1.5-4 lakhs]
Plasma(55%)
91% Water 9% solids
1% inorganic 8% organic](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-5-2048.jpg)




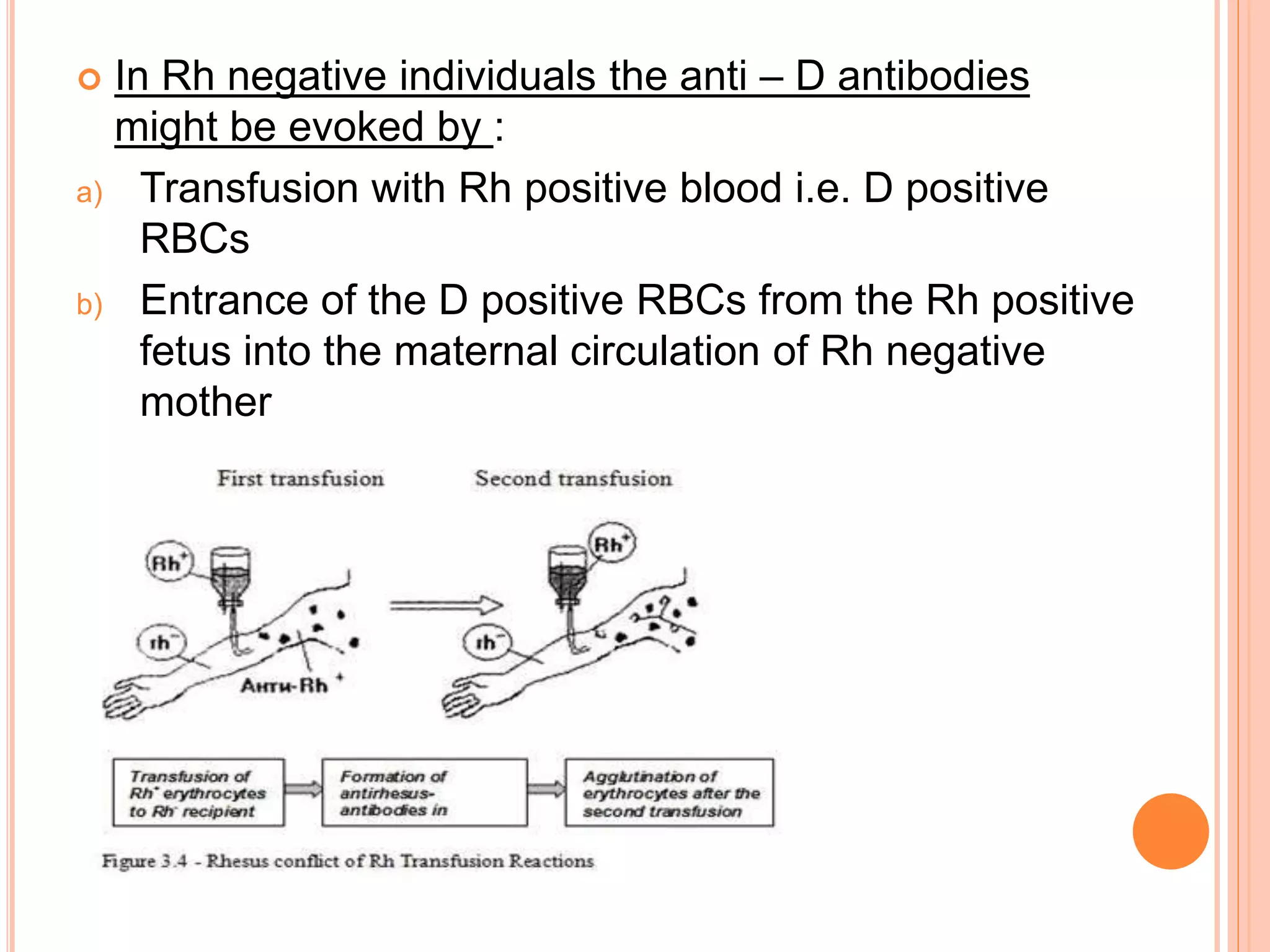
![RHESUS BLOOD GROUP
The Rh system, which includes the D, C, c, E, and e
antigens, differs from the ABO system in several ways
It is second only to the ABO system in importance in
transfusion medicine.
The Rh antigens are highly immunogenic, especially the D
antigen since these antigens are membrane-spanning
proteins, in contrast to polysaccharide moieties.
In the Rh system the antibodies are of IgG type and antigen
–antibody reaction occurs best at body temperature .[warm
antibodies]
In Rh negative individuals , anti – D antibodies are not
naturally present in the plasma](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-11-2048.jpg)






![BOMBAY BLOOD GROUP[OH GROUP]
o Rare individuals also lack the H antigen and
are designated as the “Bombay” phenotype (group
Oh). They make potent anti-H in addition to anti-A
and anti-B and must be transfused blood only from
other individuals with the Bombay phenotype.
It is observed to occur in 1 out
of every 250,000 people
It was discovered by Y.M
Bhende](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-20-2048.jpg)







![DONOR INFECTIOUS DISEASE TESTING
Hepatitis B, HbsAg and anti-core antibody
•Hepatitis C antibody
•HIV 1 and 2 antibodies
•HTLV [Human T-cell lymphotropic virus] 1 and 2
antibodies
•Serologic Test for Syphilis
•Nucleic Acid Testing (NAT) for HIV, HCV
•Detection of Bacteria in platelet products
•CMV [Cytomegalo virus] antibody for select
recipients](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-28-2048.jpg)

















![TRANSFUSION RELATED ACUTE LUNG INJURY
[TRALI]
Transfusion-related acute lung injury (TRALI) was
first recognized in 1926 and was previously known
as pulmonary hypersensitivity reaction
Pathophysiology :
TRALI’s pathogenesis revolves around the
transfusion of antibodies and/ or other non
immunologic mediators to a susceptible patient
The most frequently implicated antibodies are
human leukocyte antigen (HLA) class I, HLA class
II, and human neutrophil antibodies (HNA)5,7;
these antibodies activate the leukocytes, which bind
to the endothelium in the lungs, causing endothelial
injury and edema](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-52-2048.jpg)

![TRANSFUSION ASSOCIATED CIRCULATORY
OVERLOAD[TACO]
Transfusion-associated circulatory overload (TACO) is
generally the most common high-morbidity transfusion
reaction encountered in clinical practice
Certain patient characteristics are known to increase the
risk of TACO, including older age, renal disease, cardiac
disease, positive fluid balance, and critically ill status
Pathophysiology : Unlike the majority of transfusion
reactions, which are immunologically mediated, TACO’s
pathophysiology invokes simple physics—too much fluid
is added to the system too quickly (or in volumes that
cannot be tolerated) for the transfusion recipient.
Because the circulatory system cannot cope with the
additional volume of the transfused products, pulmonary
edema and respiratory distress result as fluid “backs up”
into the lungs](https://image.slidesharecdn.com/bloodtransfusion-191109040112/75/Blood-transfusion-54-2048.jpg)






















The document discusses blood transfusion, including its definition, history, components, and functions, explaining how blood is a vital connective tissue supplying oxygen. It details blood types such as ABO and Rh, compatibility, donor selection, screening for infectious diseases, and the principles involved in transfusion procedures. Additionally, it covers complications, indications for transfusion, and the importance of minimizing blood loss during patient management.



































































